

Efficacy and safety of isatuximab plus bortezomib, lenalidomide, and dexamethasone in patients with newly diagnosed multiple myeloma ineligible/with no immediate intent for autologous stem cell transplantation
- PMID: 37316728
- PMCID: PMC10264885
- DOI: 10.1038/s41375-023-01936-7
Efficacy and safety of isatuximab plus bortezomib, lenalidomide, and dexamethasone in patients with newly diagnosed multiple myeloma ineligible/with no immediate intent for autologous stem cell transplantation
Abstract
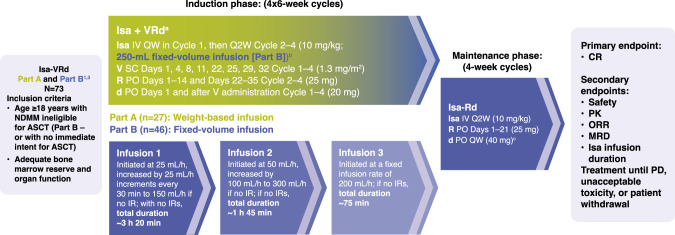
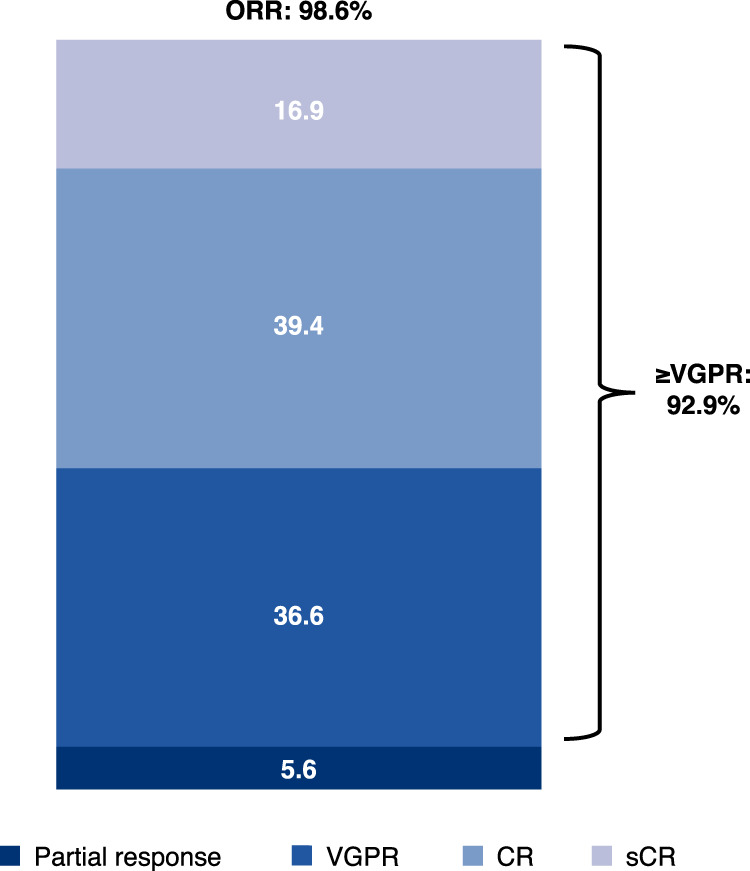
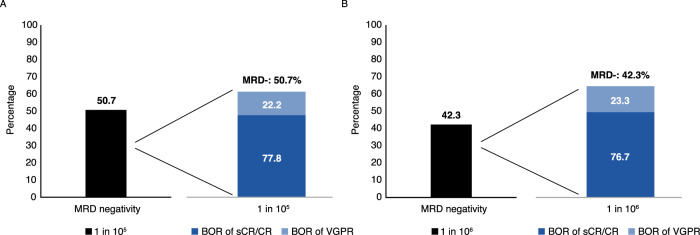
Patients with newly diagnosed multiple myeloma (NDMM) ineligible for autologous stem cell transplantation (ASCT) have lower survival rates and may benefit from frontline regimens that include novel agents. This Phase 1b study (NCT02513186) evaluated preliminary efficacy, safety, and pharmacokinetics (PK) of isatuximab, an anti-CD38 monoclonal antibody, combined with bortezomib-lenalidomide-dexamethasone (Isa-VRd) in patients with NDMM ineligible for/with no intent for immediate ASCT. Overall, 73 patients received four 6-week induction cycles of Isa-VRd, then maintenance with Isa-Rd in 4-week cycles. In the efficacy population (n = 71), the overall response rate was 98.6%, with 56.3% achieving a complete response or better (sCR/CR), and 36/71 (50.7%) patients reaching minimal residual disease negativity (10-5 sensitivity). Grade ≥3 treatment-emergent adverse events (TEAEs) occurred in 79.5% (58/73) of patients but TEAEs leading to permanent study treatment discontinuation were reported in 14 (19.2%) patients. Isatuximab PK parameters were within the previously reported range, suggesting that VRd does not alter the PK of isatuximab. These data support additional studies of isatuximab in NDMM, such as the Phase 3 IMROZ study (Isa-VRd vs VRd).
© 2023. The Author(s).
Conflict of interest statement
EMO: Honoraria – Amgen, BMS/Celgene, GSK, Janssen, MSD, Oncopeptides, Sanofi, Takeda. AP: Honoraria – AbbVie, Amgen, BMS/Celgene, GSK, Janssen, Sanofi, Takeda. PB: nothing to disclose. JFSM: Honoraria – AbbVie, Amgen, BMS, Celgene, GSK, Haemalogix, Janssen, Karyopharm, MSD, Novartis, Regeneron, Roche, Sanofi, SecuraBio, Takeda. IWB: nothing to disclose. LK: Honoraria – AbbVie, Amgen, Celgene, Janssen, Sanofi, Takeda; Advisory Role: Amgen, Celgene, GSK, Janssen, Takeda. JM-L: Honoraria – Janssen, BMS, Incyte, Roche, Novartis, Amgen, Adaptive, Gilead, Sanofi. WP: nothing to disclose. SB: Honoraria – Janssen, Takeda, Amgen, Sanofi, Celgene, Oncopeptides, GSK, Bristol Myers Squibb. MM: nothing to disclose. M-VM: Honoraria – Sanofi. PR-O: Honoraria – Celgene-BMS, Janssen, Sanofi, AbbVie, GSK, Oncopeptides, Kite Pharma, Amgen. LD, SM, and TF are employed by Sanofi and may hold stock and/or stock options in the company Sanofi. NLR and MG are contractors for Sanofi on behalf of Altran and Excelya. PM: Consulting – AbbVie, Amgen, Celgene, Jansen, Oncopeptides, Sanofi; Honoraria – AbbVie, Amgen, Celgene, Janssen, Oncopeptides, Sanofi; Advisory Role – AbbVie, Amgen, Celgene, Janssen, Oncopeptides, Sanofi.
Figures

References
-
- Avet-Loiseau H, Ludwig H, Landgren O, Paiva B, Morris C, Yang H, et al. Minimal residual disease status as a surrogate endpoint for progression-free survival in newly diagnosed multiple myeloma studies: a meta-analysis. Clin Lymphoma Myeloma Leuk. 2020;20:e30–e7. doi: 10.1016/j.clml.2019.09.622. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
