

Additional value of cardiac magnetic resonance feature tracking parameters for the evaluation of the arrhythmic risk in patients with mitral valve prolapse
- PMID: 37316826
- PMCID: PMC10268415
- DOI: 10.1186/s12968-023-00944-x
Additional value of cardiac magnetic resonance feature tracking parameters for the evaluation of the arrhythmic risk in patients with mitral valve prolapse
Abstract
Objectives: The identification of patients with mitral valve prolapse (MVP) presenting high arrhythmic risk remains challenging. Cardiovascular Magnetic Resonance (CMR) feature tracking (FT) may improve risk stratification. We analyzed the role of CMR-FT parameters in relation to the incidence of complex ventricular arrhythmias (cVA) in patients with MVP and mitral annular disjunction (MAD).
Methods: 42 patients with MVP and MAD who underwent 1.5 T CMR were classified as MAD-cVA (n = 23, 55%) in case of cVA diagnosed on a 24-h Holter monitoring and as MAD-noVA in the absence of cVA (n = 19, 45%). MAD length, late gadolinium enhancement (LGE), basal segments myocardial extracellular volume (ECV) and CMR-FT were assessed.
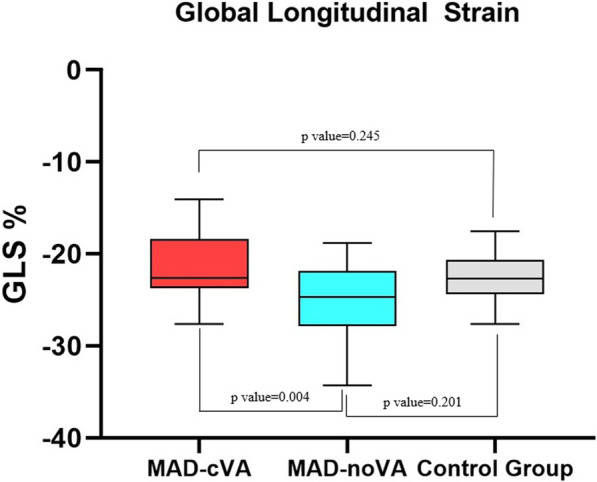
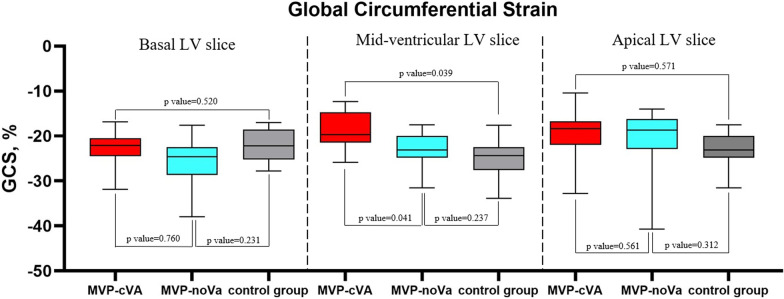
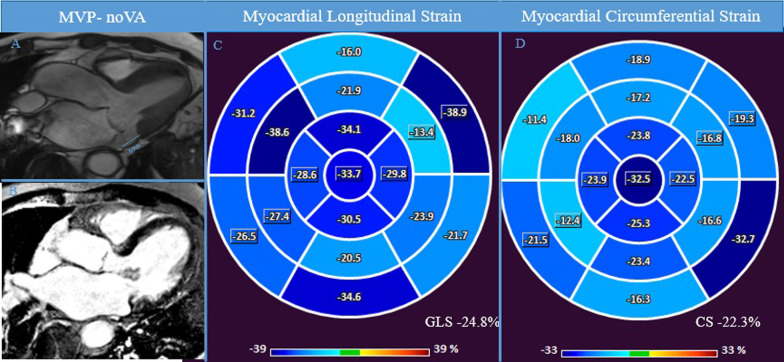
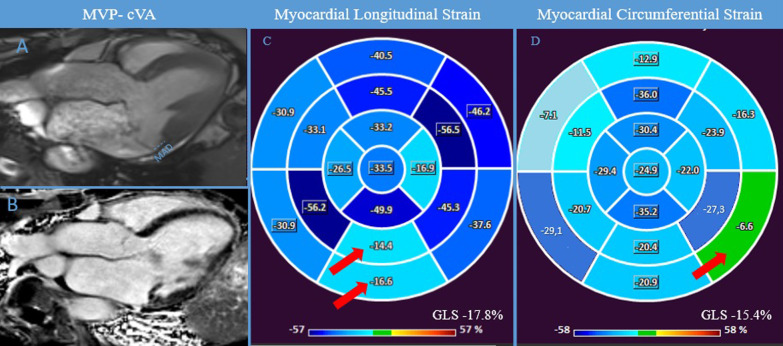
Results: LGE was more frequent in the MAD-cVA group in comparison with the MAD-noVA group (78% vs 42%, p = 0.002) while no difference was observed in terms of basal ECV. Global longitudinal strain (GLS) was reduced in MAD-cVA compared to MAD-noVA (- 18.2% ± 4.6% vs - 25.1% ± 3.1%, p = 0.004) as well as global circumferential strain (GCS) at the mid-ventricular level (- 17.5% ± 4.7% vs - 21.6% ± 3.1%, p = 0.041). Univariate analysis identified as predictors of the incidence of cVA: GCS, circumferential strain (CS) in the basal and mid infero-lateral wall, GLS, regional longitudinal strain (LS) in the basal and mid-ventricular inferolateral wall. Reduced GLS [Odd ratio (OR):1.56 (confidence interval (CI) 95%: 1.45-2.47; p < 0.001)] and regional LS in the basal inferolateral wall [OR: 1.62 (CI 95%: 1.22-2.13; p < 0.001)] remained independent prognostic factors in multivariate analysis.
Conclusion: In patients with MVP and MAD, CMR-FT parameters are correlated with the incidence of cVA and may be of interest in arrhythmic risk stratification.
Keywords: Cardiovascular magnetic resonance; Interstitial fibrosis; Mitral annular disjunction; Mitral valve prolapse; Strain.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they do not have any competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
