

Comparison of aortic stiffness and hypertension in repaired coarctation patients with a bicuspid versus a tricuspid aortic valve
- PMID: 37316842
- PMCID: PMC10268521
- DOI: 10.1186/s12968-023-00941-0
Comparison of aortic stiffness and hypertension in repaired coarctation patients with a bicuspid versus a tricuspid aortic valve
Abstract
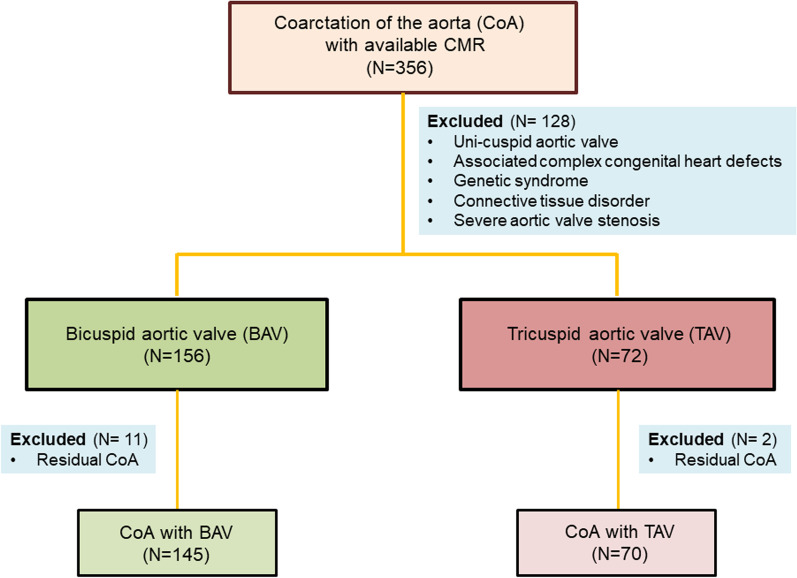
Background: Coarctation of the aorta (COA) is associated with reduced aortic distensibility and systemic hypertension (HTN). 60-85% of COA patients have a bicuspid aortic valve (BAV). It is not known if the presence of a BAV accentuates the aortopathy and HTN in CoA patients. We examined whether patients with COA and a BAV had lower aortic distensibility by CMR, and a higher prevalence of systemic HTN compared with COA patients with a tricuspid aortic valve (TAV).
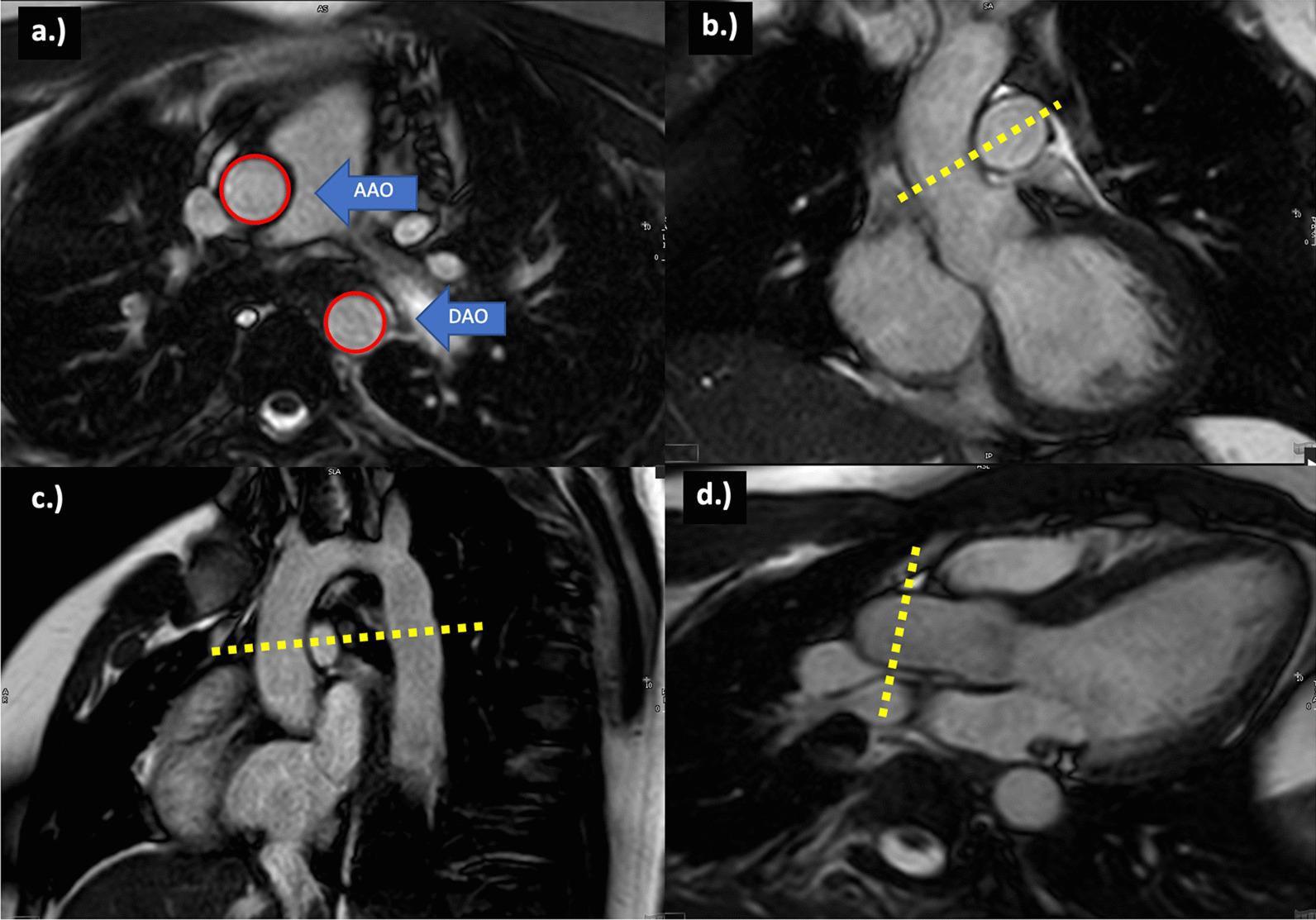
Methods: In successfully repaired COA patients excluding those with residual COA, ascending aorta (AAO) and descending aorta (DAO) distensibility was calculated by CMR. HTN was assessed using standard pediatric and adult criteria.
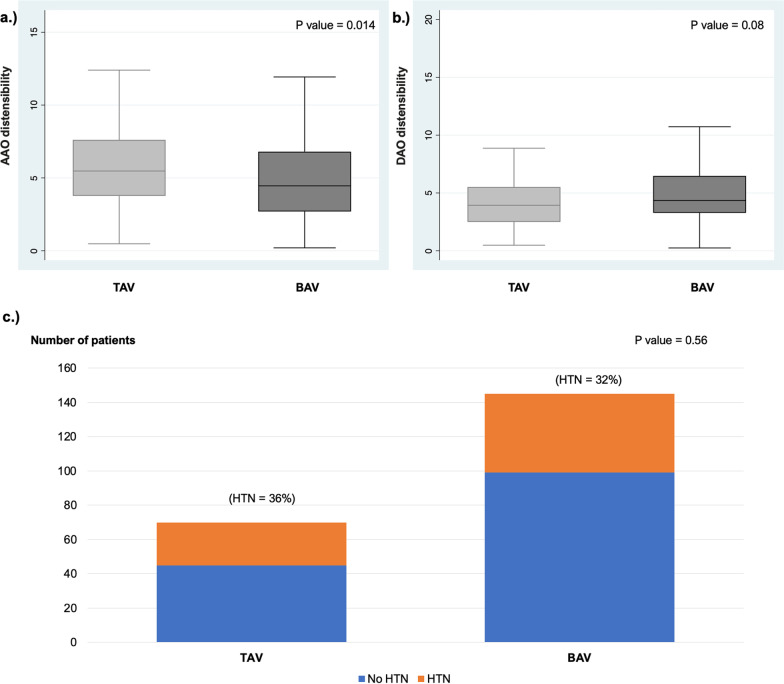
Results: Among 215 COA patients (median age 25.3 years), 67% had a BAV, and 33% had a TAV. Median AAO distensibility z-score was lower in the BAV group (- 1.2 versus - 0.7; p = 0.014) but DAO distensibility was similar in BAV and TAV patients. HTN prevalence was similar in BAV (32%) and TAV groups (36%, p = 0.56). On multivariable analysis controlling for confounders, HTN was not associated with BAV but was associated with male gender (p = 0.003) and older age at follow-up (p = 0.004).
Conclusions: In young adults with treated COA, those with a BAV had stiffer AAO compared to those with a TAV, but DAO stiffness was similar. HTN was not related to BAV. These results suggest that although the presence of a BAV in COA exacerbates the AAO aortopathy, it does not exacerbate the more generalized vascular dysfunction and associated HTN.
Keywords: Aortic dilation; Bicuspid aortic valve; Cardiac MRI; Coarctation of the aorta; Vascular stiffness.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Loffredo CA, Chokkalingam A, Sill AM, Boughman JA, Clark EB, Scheel J, Brenner JI. Prevalence of congenital cardiovascular malformations among relatives of infants with hypoplastic left heart, coarctation of the aorta, and d-transposition of the great arteries. Am J Med Genet Part A. 2004;124aa:225–230. doi: 10.1002/ajmg.a.20366. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
