

Assessing real-world gait with digital technology? Validation, insights and recommendations from the Mobilise-D consortium
- PMID: 37316858
- PMCID: PMC10265910
- DOI: 10.1186/s12984-023-01198-5
Assessing real-world gait with digital technology? Validation, insights and recommendations from the Mobilise-D consortium
Erratum in
-
Correction: Assessing real-world gait with digital technology? Validation, insights and recommendations from the Mobilise-D consortium.J Neuroeng Rehabil. 2024 May 3;21(1):71. doi: 10.1186/s12984-024-01361-6. J Neuroeng Rehabil. 2024. PMID: 38702693 Free PMC article. No abstract available.
Abstract
Background: Although digital mobility outcomes (DMOs) can be readily calculated from real-world data collected with wearable devices and ad-hoc algorithms, technical validation is still required. The aim of this paper is to comparatively assess and validate DMOs estimated using real-world gait data from six different cohorts, focusing on gait sequence detection, foot initial contact detection (ICD), cadence (CAD) and stride length (SL) estimates.
Methods: Twenty healthy older adults, 20 people with Parkinson's disease, 20 with multiple sclerosis, 19 with proximal femoral fracture, 17 with chronic obstructive pulmonary disease and 12 with congestive heart failure were monitored for 2.5 h in the real-world, using a single wearable device worn on the lower back. A reference system combining inertial modules with distance sensors and pressure insoles was used for comparison of DMOs from the single wearable device. We assessed and validated three algorithms for gait sequence detection, four for ICD, three for CAD and four for SL by concurrently comparing their performances (e.g., accuracy, specificity, sensitivity, absolute and relative errors). Additionally, the effects of walking bout (WB) speed and duration on algorithm performance were investigated.
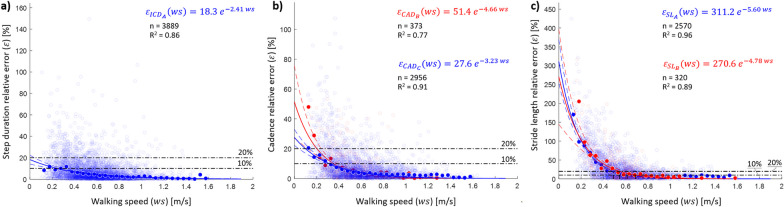
Results: We identified two cohort-specific top performing algorithms for gait sequence detection and CAD, and a single best for ICD and SL. Best gait sequence detection algorithms showed good performances (sensitivity > 0.73, positive predictive values > 0.75, specificity > 0.95, accuracy > 0.94). ICD and CAD algorithms presented excellent results, with sensitivity > 0.79, positive predictive values > 0.89 and relative errors < 11% for ICD and < 8.5% for CAD. The best identified SL algorithm showed lower performances than other DMOs (absolute error < 0.21 m). Lower performances across all DMOs were found for the cohort with most severe gait impairments (proximal femoral fracture). Algorithms' performances were lower for short walking bouts; slower gait speeds (< 0.5 m/s) resulted in reduced performance of the CAD and SL algorithms.
Conclusions: Overall, the identified algorithms enabled a robust estimation of key DMOs. Our findings showed that the choice of algorithm for estimation of gait sequence detection and CAD should be cohort-specific (e.g., slow walkers and with gait impairments). Short walking bout length and slow walking speed worsened algorithms' performances. Trial registration ISRCTN - 12246987.
Keywords: Accelerometer; Algorithms; Cadence; DMOs; Digital health; Real-world gait; SL; Validation; Walking; Wearable sensor.
© 2023. The Author(s).
Conflict of interest statement
A. Mueller and F. Kluge are employees of, and may hold stock in, Novartis. B. Eskofier reports consulting activities with adidas AG, Siemens AG, Siemens Healthineers AG, WSAudiology GmbH outside of the study. He is a shareholder in Portabiles HealthCare Technologies GmbH. In addition, Dr. Eskofier holds a patent related to gait assessment. H. Sillén is an employee of, and may hold stock in, AstraZeneca. M. Froelich is an employee of Grunenthal. L. Palmerini and L. Chiari are co-founders and own shares of mHealth Technologies (
Figures



References
-
- Van Kan GA, Rolland Y, Andrieu S, Bauer J, Beauchet O, Bonnefoy M, et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) Task Force. J Nutr Health Aging. 2009;13(10):881–9. doi: 10.1007/s12603-009-0246-z. - DOI - PubMed
-
- Henderson EJ, Lord SR, Brodie MA, Gaunt DM, Lawrence AD, Close JC, et al. Rivastigmine for gait stability in patients with Parkinson’s disease (ReSPonD): a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Neurol. 2016;15(3):249–258. doi: 10.1016/S1474-4422(15)00389-0. - DOI - PubMed
-
- Mirelman A, Rochester L, Maidan I, Del Din S, Alcock L, Nieuwhof F, et al. Addition of a non-immersive virtual reality component to treadmill training to reduce fall risk in older adults (V-TIME): a randomised controlled trial. Lancet. 2016;388(10050):1170–1182. doi: 10.1016/S0140-6736(16)31325-3. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
