

Time-dependent changes in P2Y12 reaction unit values for predicting the different types of cardiovascular events in patients with ischemic heart disease
- PMID: 37318650
- PMCID: PMC10465654
- DOI: 10.1007/s00380-023-02279-0
Time-dependent changes in P2Y12 reaction unit values for predicting the different types of cardiovascular events in patients with ischemic heart disease
Abstract
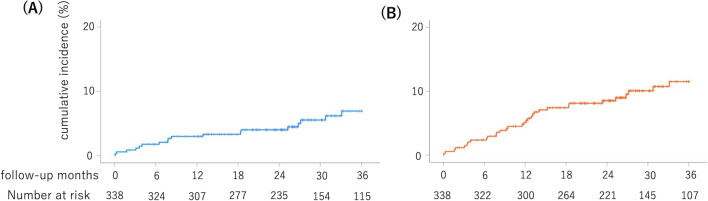
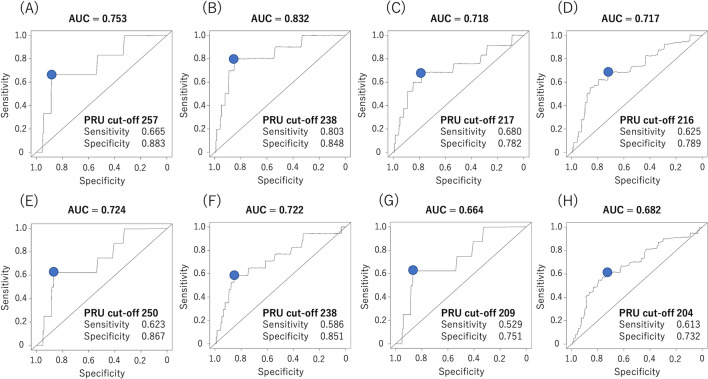
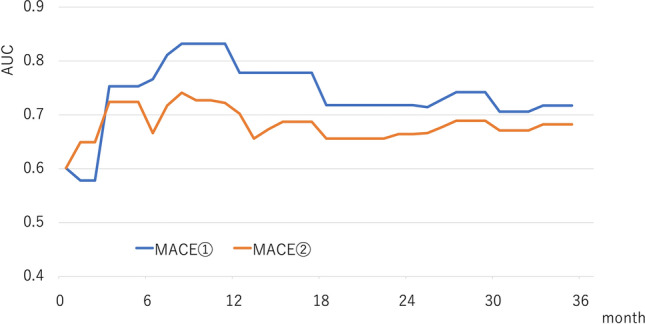
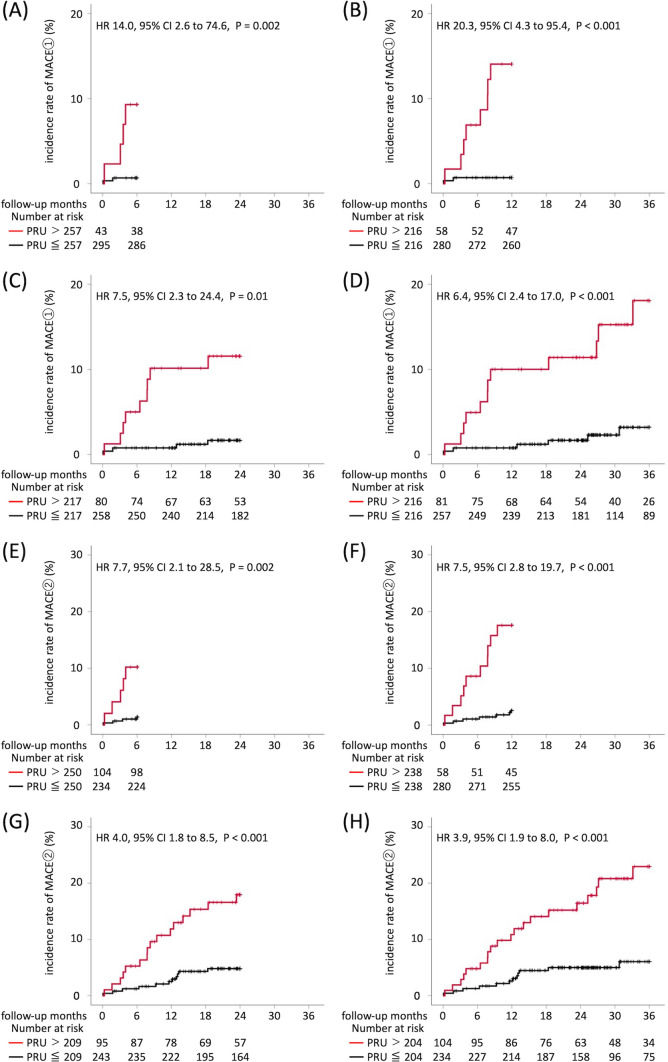
Several studies have investigated the association between P2Y12 reaction unit (PRU) value and major adverse cardiovascular events (MACEs) in patients with ischemic heart disease, but there is no well-established consensus on the utility of PRU value. Furthermore, the optimal PRU cut-off value varied with studies. One reason may be that the endpoints and observation periods differed, depending on the study. This study aimed to investigate the optimal cut-off and predictive ability of the PRU value for predicting cardiovascular events, while considering different endpoints and observation periods. We surveyed a total of 338 patients receiving P2Y12 inhibitors and measured PRU during cardiac catheterization. Using time-dependent receiver operating characteristic analysis, we evaluated the cut-off and area under curve (AUC) of the PRU value for two MACEs (MACE ①: composite of death, myocardial infarction, stent thrombosis, and cerebral infarction; MACE ②: composite of MACE ① and target vessel revascularization) at 6, 12, 24 and 36 months after cardiac catheterization. MACE ① occurred in 18 cases and MACE ② in 32 cases. The PRU cut-off values at 6, 12, 24, and 36 months were 257, 238, 217, and 216, respectively, for MACE ① and 250, 238, 209, and 204, respectively, for MACE ②. The AUCs at 6, 12, 24, and 36 months were 0.753, 0.832, 0.718, and 0.717, respectively, for MACE ① and 0.724, 0.722, 0.664, and 0.682, respectively, for MACE ②. The optimal cut-off and predictive ability of PRU values for cardiovascular events varied depending on different endpoints and duration of the observation periods. A relatively high PRU value is effective for short-term event suppression, but a low value is required for long-term event suppression.
Keywords: Major adverse cardiovascular event; Optimal cut-off value; P2Y12 reaction unit; Time-dependent receiver-operating characteristic analysis.
© 2023. The Author(s).
Conflict of interest statement
Takayuki Ogawa reports that there are no relevant conflicts of interest. Outside the submitted work, Takayuki Ogawa received personal fees from Terumo Co. and personal fees from Kaneka Co. Makoto Kawai has no conflict of interest and reports that there are no relevant conflicts of interest. Outside the submitted work, Makoto Kawai received scholarship donations from Daiichi Sankyo Co., Ltd. Michihiro Yoshimura reports that there are no relevant conflicts of interest. Outside the submitted work, Michihiro Yoshimura received lecture fees from Mochida Pharmaceutical Co., Ltd., Daiichi Sankyo Co., Ltd., Mitsubishi Tanabe Pharma Corporation, Pfizer Japan Inc., Kowa Co., Ltd., and Astra Zeneca Plc., as well as scholarship donations from Teijin Pharma Ltd. and Shionogi & Co., Ltd. The other authors have no conflict of interest.
Figures
Similar articles
-
The effect of correcting VerifyNow P2Y12 assay results for hematocrit in patients undergoing percutaneous coronary interventions.J Thromb Haemost. 2017 Apr;15(4):618-623. doi: 10.1111/jth.13642. Epub 2017 Feb 25. J Thromb Haemost. 2017. PMID: 28135786
-
High post-clopidogrel platelet reactivity assessed by a point-of-care assay predicts long-term clinical outcomes in patients with ST-segment elevation myocardial infarction who underwent primary coronary stenting.Int J Cardiol. 2013 Sep 1;167(5):1877-81. doi: 10.1016/j.ijcard.2012.04.154. Epub 2012 Jun 9. Int J Cardiol. 2013. PMID: 22682702
-
Optimal cutoff value of P2Y12 reaction units to prevent major adverse cardiovascular events in the acute periprocedural period: post-hoc analysis of the randomized PRASFIT-ACS study.Int J Cardiol. 2015 Mar 1;182:541-8. doi: 10.1016/j.ijcard.2015.01.026. Epub 2015 Jan 8. Int J Cardiol. 2015. PMID: 25679803
-
Consensus and update on the definition of on-treatment platelet reactivity to adenosine diphosphate associated with ischemia and bleeding.J Am Coll Cardiol. 2013 Dec 17;62(24):2261-73. doi: 10.1016/j.jacc.2013.07.101. Epub 2013 Sep 27. J Am Coll Cardiol. 2013. PMID: 24076493
-
Crushed/chewed administration of potent P2Y12 inhibitors in ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention: Systematic review and meta-analysis.Platelets. 2022 Jul 4;33(5):679-686. doi: 10.1080/09537104.2021.1974370. Epub 2021 Sep 2. Platelets. 2022. PMID: 34472997
Cited by
-
Cut-off values of Geriatric Nutritional Risk Index for cardiovascular events in Japanese patients with acute myocardial infarction.Heart Vessels. 2025 Mar;40(3):191-202. doi: 10.1007/s00380-024-02455-w. Epub 2024 Sep 13. Heart Vessels. 2025. PMID: 39269471 Free PMC article.
References
-
- Bonello L, Tantry US, Marcucci R, Blindt R, Angiolillo DJ, Becker R, Bhatt DL, Cattaneo M, Collet JP, Cuisset T, Gachet C, Montalescot G, Jennings LK, Kereiakes D, Sibbing D, Trenk D, Van Werkum JW, Paganelli F, Price MJ, Waksman R, Gurbel PA, Working Group on High On-Treatment Platelet R Consensus and future directions on the definition of high on-treatment platelet reactivity to adenosine diphosphate. J Am Coll Cardiol. 2010;56(12):919–933. doi: 10.1016/j.jacc.2010.04.047. - DOI - PubMed
-
- Malinin A, Pokov A, Spergling M, Defranco A, Schwartz K, Schwartz D, Mahmud E, Atar D, Serebruany V. Monitoring platelet inhibition after clopidogrel with the VerifyNow-P2Y12(R) rapid analyzer: the VERIfy Thrombosis risk ASsessment (VERITAS) study. Thromb Res. 2007;119(3):277–284. doi: 10.1016/j.thromres.2006.01.019. - DOI - PubMed
-
- Varenhorst C, James S, Erlinge D, Braun OO, Brandt JT, Winters KJ, Jakubowski JA, Olofsson S, Wallentin L, Siegbahn A. Assessment of P2Y(12) inhibition with the point-of-care device VerifyNow P2Y12 in patients treated with prasugrel or clopidogrel coadministered with aspirin. Am Heart J. 2009;157(3):562 e561–569. doi: 10.1016/j.ahj.2008.11.021. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
