

Ambulatory daytime blood pressure versus tonometric blood pressure measurements in the laboratory: effect of posture
- PMID: 37318783
- PMCID: PMC10309093
- DOI: 10.1097/MBP.0000000000000651
Ambulatory daytime blood pressure versus tonometric blood pressure measurements in the laboratory: effect of posture
Abstract
Objective: To compare blood pressure (BP) in tonometric radial artery recordings during passive head-up tilt with ambulatory recordings and evaluate possible laboratory cutoff values for hypertension.
Methods: Laboratory BP and ambulatory BP were recorded in normotensive (n = 69), unmedicated hypertensive (n = 190), and medicated hypertensive (n = 151) subjects.
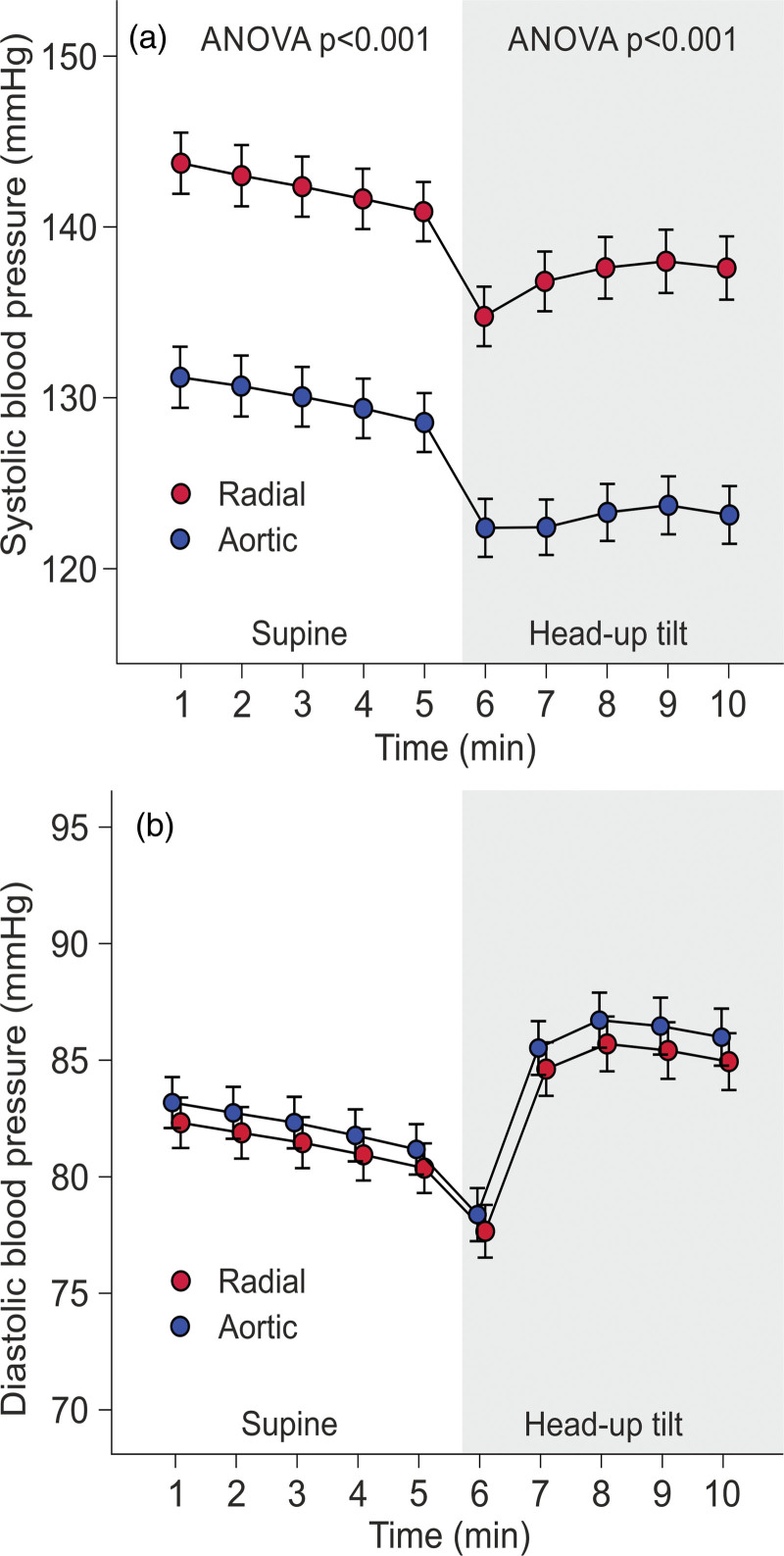
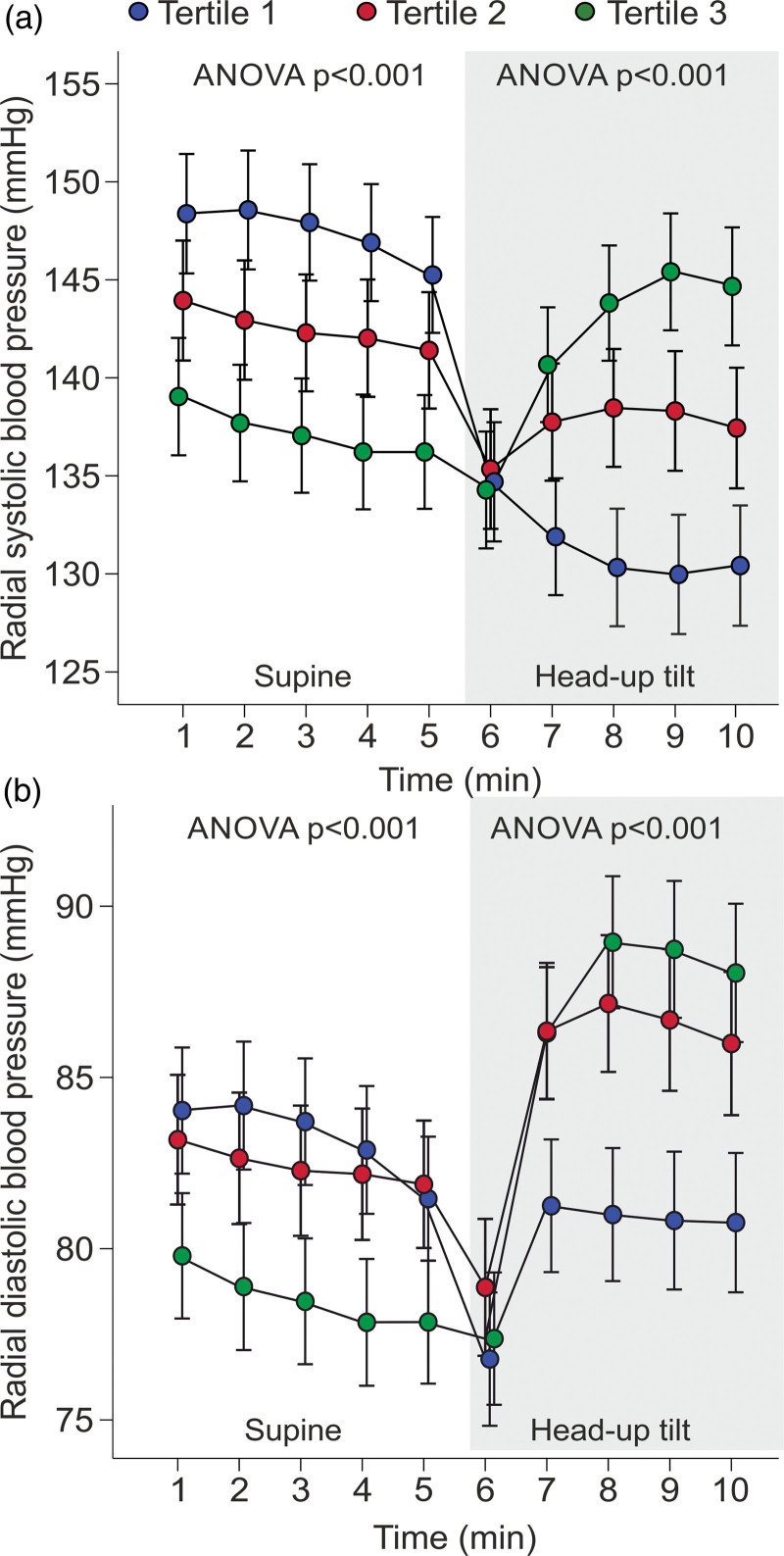
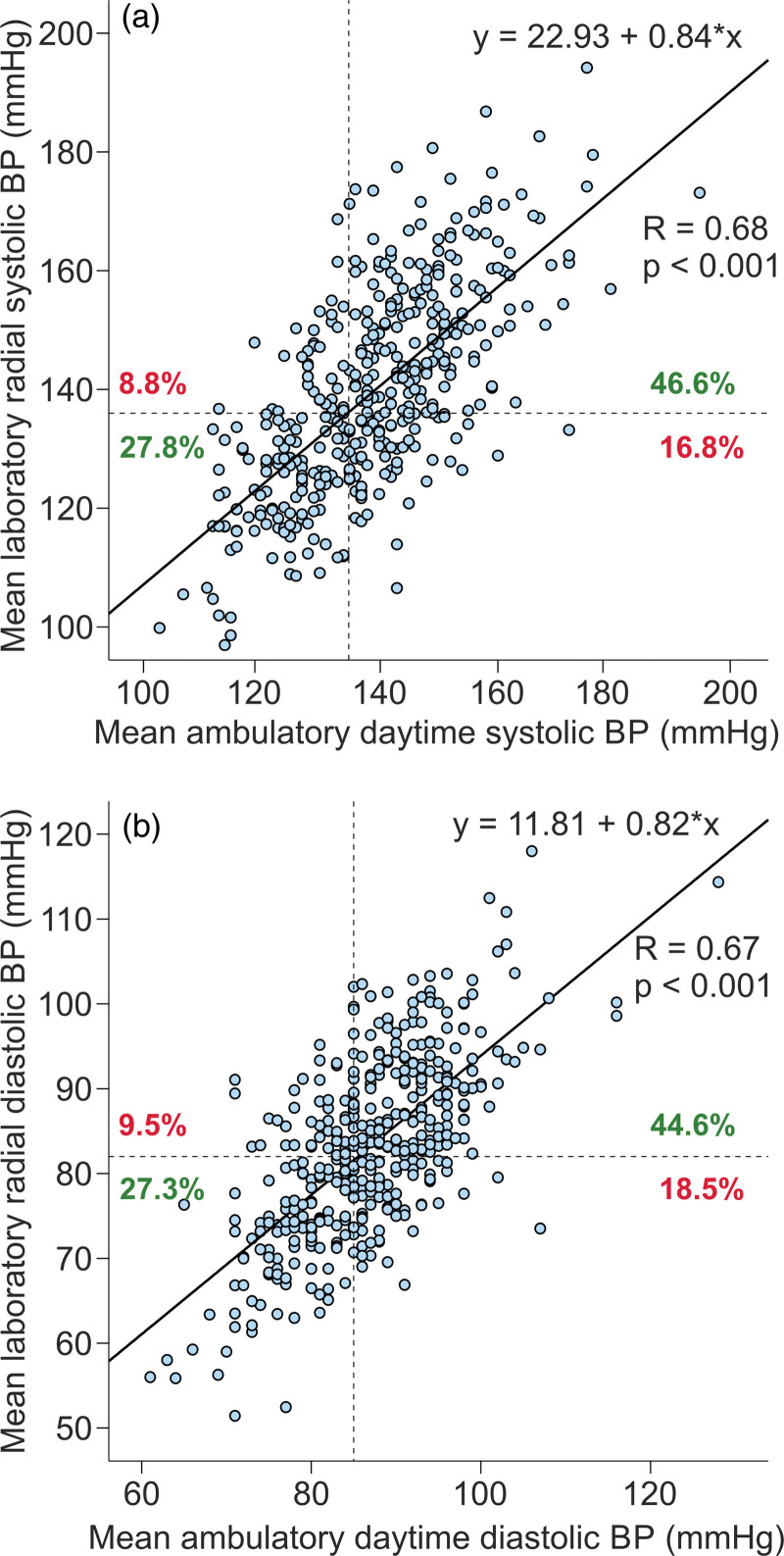
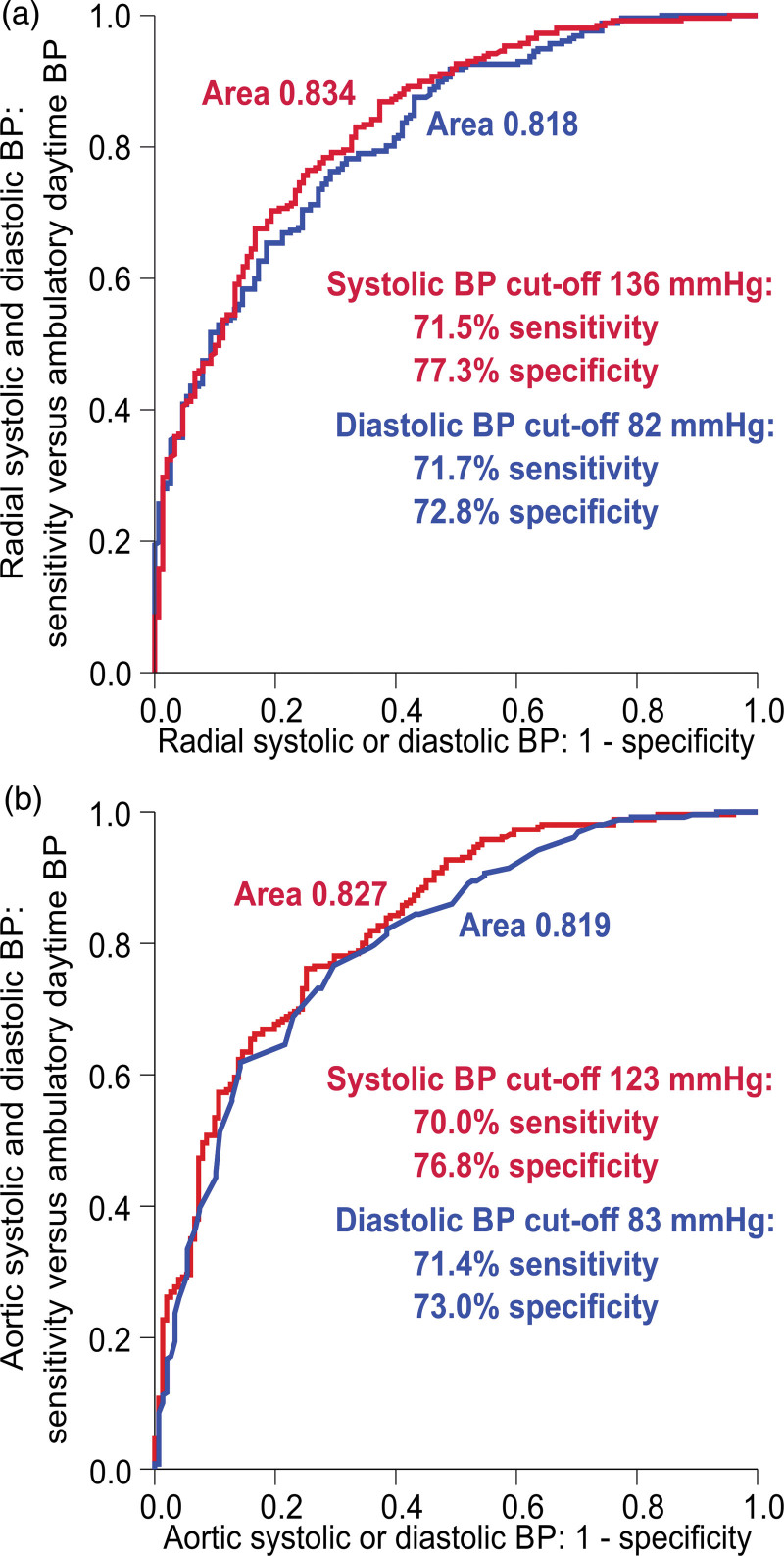
Results: Mean age was 50.2 years, BMI 27.7 kg/m 2 , ambulatory daytime BP 139/87 mmHg, and 276 were male (65%). As supine-to-upright changes in SBP ranged from -52 to +30 mmHg, and in DBP from -21 to +32 mmHg, the mean values of BP supine and upright measurements were compared with ambulatory BP. The mean(supine+upright) systolic laboratory BP was corresponding to ambulatory level (difference +1 mmHg), while mean(supine+upright) DBP was 4 mmHg lower ( P < 0.05) than ambulatory value. Correlograms indicated that laboratory 136/82 mmHg corresponded to ambulatory 135/85 mmHg. When compared with ambulatory 135/85 mmHg, the sensitivity and specificity of laboratory 136/82 mmHg to define hypertension were 71.5% and 77.3% for SBP, and 71.7% and 72.8%, for DBP, respectively. The laboratory cutoff 136/82 mmHg classified 311/410 subjects similarly to ambulatory BP as normotensive or hypertensive, 68 were hypertensive only in ambulatory, while 31 were hypertensive only in laboratory measurements.
Conclusion: BP responses to upright posture were variable. When compared with ambulatory BP, mean(supine+upright) laboratory cutoff 136/82 mmHg classified 76% of subjects similarly as normotensive or hypertensive. In the remaining 24% the discordant results may be attributed to white-coat or masked hypertension, or higher physical activity during out-of-office recordings.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. .; ESC Scientific Document Group. 2018 ESC/ESH guidelines for the management of arterial hypertension. Eur Heart J 2018; 39:3021–3104. - PubMed
-
- Picone DS, Schultz MG, Otahal P, Aakhus S, Al-Jumaily AM, Black JA, et al. . Accuracy of cuff-measured blood pressure. J Am Coll Cardiol 2017; 70:572–586. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
