

Analysis of Race and Ethnicity, Socioeconomic Factors, and Tooth Decay Among US Children
- PMID: 37318807
- PMCID: PMC10273024
- DOI: 10.1001/jamanetworkopen.2023.18425
Analysis of Race and Ethnicity, Socioeconomic Factors, and Tooth Decay Among US Children
Abstract
Importance: While large oral health disparities remain by race and ethnicity among children, the associations of race, ethnicity, and mediating factors with oral health outcomes are poorly characterized. Identifying the pathways that explain these disparities would be critical to inform policies to effectively reduce them.
Objective: To measure racial and ethnic disparities in the risk of developing tooth decay and quantify relative contributions of factors mediating the observed disparities among US children.
Design, setting, and participants: This retrospective cohort study used electronic health records of US children from 2014 to 2020 to measure racial and ethnic disparities in the risk of tooth decay. Elastic net regularization was used to select variables to be included in the model among medical conditions, dental procedure types, and individual- and community-level socioeconomic factors. Data were analyzed from January 9 to April 28, 2023.
Exposures: Race and ethnicity of children.
Main outcomes and measures: The main outcome was diagnosis of tooth decay in either deciduous or permanent teeth, defined as at least 1 decayed, filled, or missing tooth due to caries. An Anderson-Gill model, a time-to-event model for recurrent tooth decay events with time-varying covariates, stratified by age groups (0-5, 6-10, and 11-18 years) was estimated. A nonlinear multiple additive regression tree-based mediation analysis quantified the relative contributions of factors underlying the observed racial and ethnic disparities.
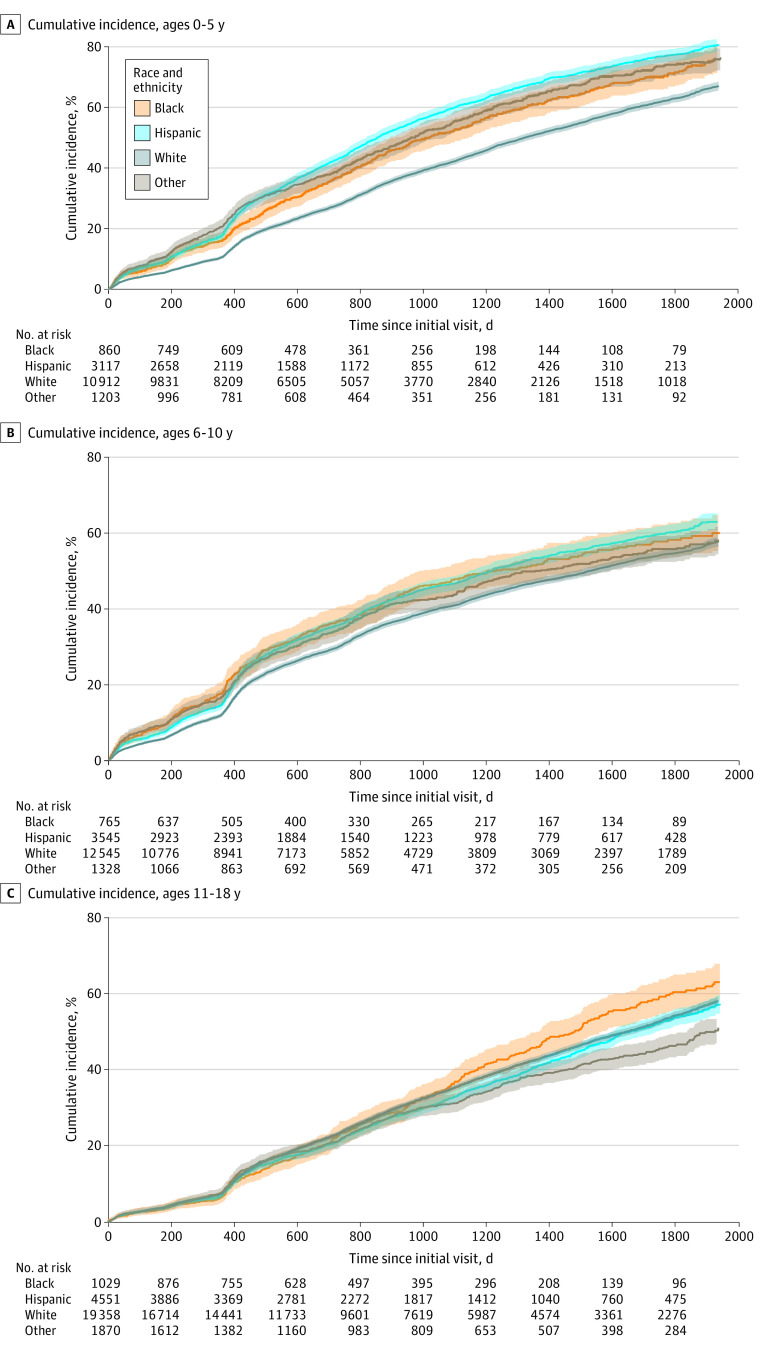
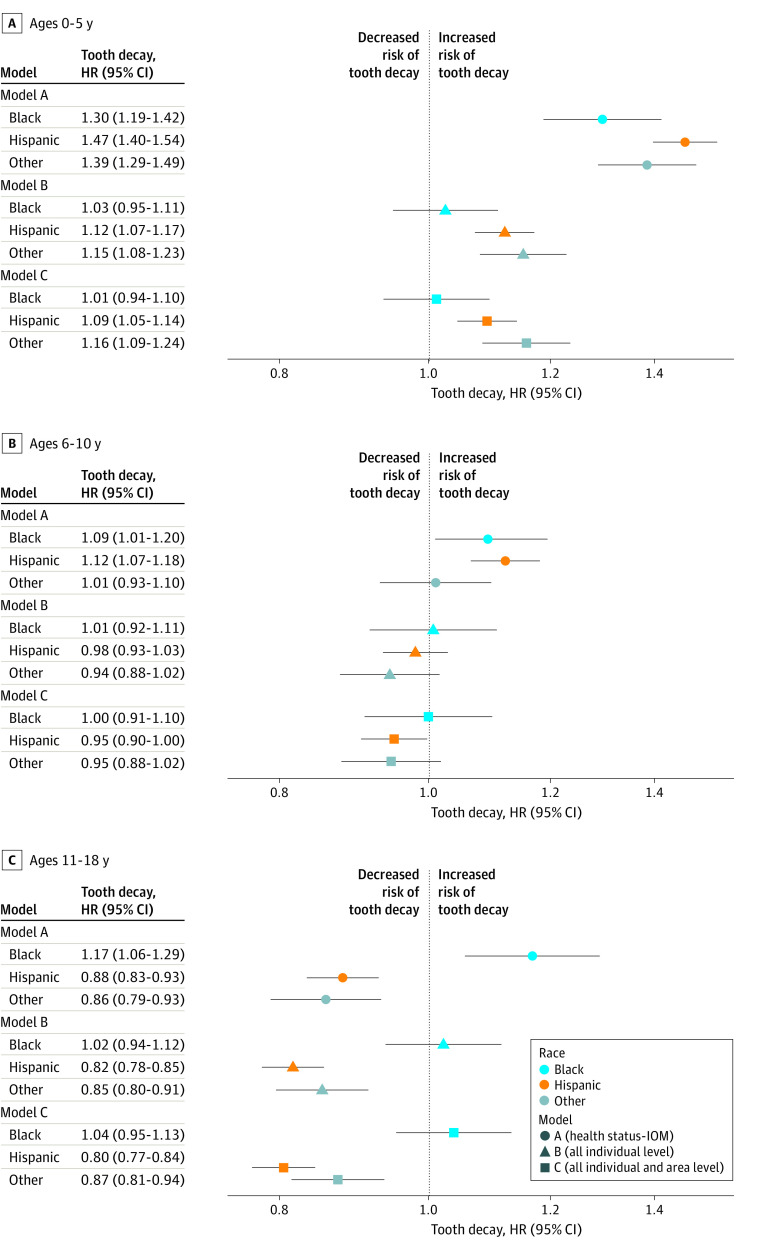
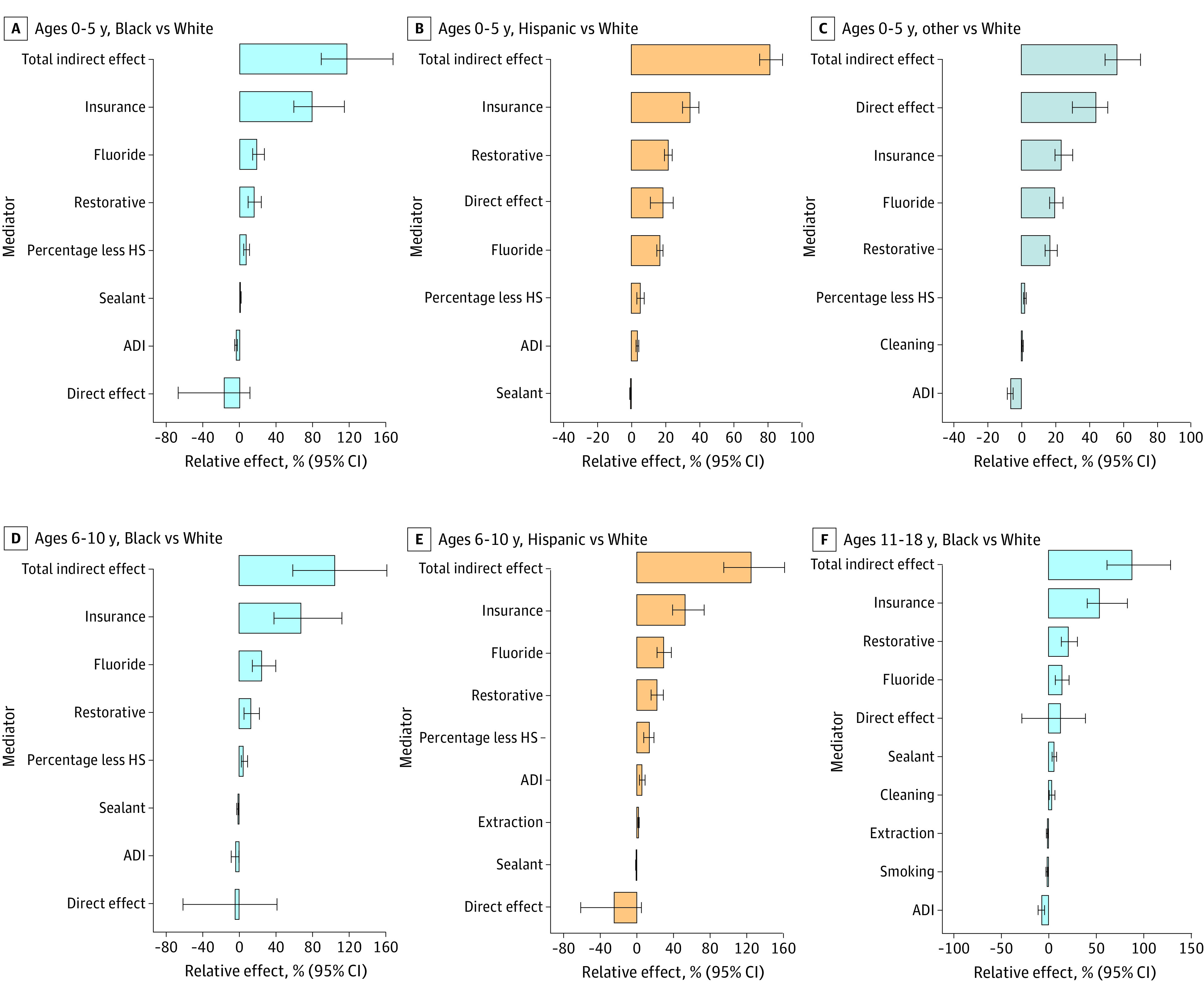
Results: Among 61 083 children and adolescents aged 0 to 18 years at baseline (mean [SD] age, 9.9 [4.6] years; 30 773 [50.4%] female), 2654 Black individuals (4.3%), 11 213 Hispanic individuals (18.4%), 42 815 White individuals (70.1%), and 4401 individuals who identified as another race (eg, American Indian, Asian, and Hawaiian and Pacific Islander) (7.2%) were identified. Larger racial and ethnic disparities were observed among children aged 0 to 5 years compared with other age groups (Hispanic children: adjusted hazard ratio [aHR], 1.47; 95% CI, 1.40-1.54; Black children: aHR, 1.30; 95% CI, 1.19-1.42; other race children: aHR, 1.39; 95% CI, 1.29-1.49), compared with White children. For children aged 6 to 10 years, higher risk of tooth decay was observed for Black children (aHR, 1.09; 95% CI, 1.01-1.19) and Hispanic children (aHR, 1.12; 95% CI, 1.07-1.18) compared with White children. For adolescents aged 11 to 18 years, a higher risk of tooth decay was observed only in Black adolescents (aHR, 1.17; 95% CI, 1.06-1.30). A mediation analysis revealed that the association of race and ethnicity with time to first tooth decay became negligible, except for Hispanic and children of other race aged 0 to 5 years, suggesting that mediators explained most of the observed disparities. Insurance type explained the largest proportion of the disparity, ranging from 23.4% (95% CI, 19.8%-30.2%) to 78.9% (95% CI, 59.0%-114.1%), followed by dental procedures (receipt of topical fluoride and restorative procedures) and community-level factors (education attainment and Area Deprivation Index).
Conclusions: In this retrospective cohort study, large proportions of disparities in time to first tooth decay associated with race and ethnicity were explained by insurance type and dental procedure types among children and adolescents. These findings can be applied to develop targeted strategies to reduce oral health disparities.
Conflict of interest statement
Figures
Similar articles
-
State Variation in Racial and Ethnic Disparities in Incidence of Triple-Negative Breast Cancer Among US Women.JAMA Oncol. 2023 May 1;9(5):700-704. doi: 10.1001/jamaoncol.2022.7835. JAMA Oncol. 2023. PMID: 36862439 Free PMC article.
-
Declination of Treatment, Racial and Ethnic Disparity, and Overall Survival in US Patients With Breast Cancer.JAMA Netw Open. 2024 May 1;7(5):e249449. doi: 10.1001/jamanetworkopen.2024.9449. JAMA Netw Open. 2024. PMID: 38722630 Free PMC article.
-
Associations Between Race/Ethnicity and US Childhood and Adolescent Cancer Survival by Treatment Amenability.JAMA Pediatr. 2020 May 1;174(5):428-436. doi: 10.1001/jamapediatrics.2019.6074. JAMA Pediatr. 2020. PMID: 32091555 Free PMC article.
-
Race and Ethnicity Representation in Phase 2/3 Oncology Clinical Trial Publications: A Systematic Review.JAMA Health Forum. 2024 Jun 7;5(6):e241388. doi: 10.1001/jamahealthforum.2024.1388. JAMA Health Forum. 2024. PMID: 38848090 Free PMC article.
-
Quantification of race/ethnicity representation in Alzheimer's disease neuroimaging research in the USA: a systematic review.Commun Med (Lond). 2023 Jul 25;3(1):101. doi: 10.1038/s43856-023-00333-6. Commun Med (Lond). 2023. PMID: 37491471 Free PMC article. Review.
Cited by
-
Race, Ethnicity, and Intensive Care Utilization for Common Pediatric Diagnoses: U.S. Pediatric Health Information System 2019 Database Study.Pediatr Crit Care Med. 2024 Sep 1;25(9):828-837. doi: 10.1097/PCC.0000000000003487. Epub 2024 Feb 29. Pediatr Crit Care Med. 2024. PMID: 38421235
-
Oral Health and Caries Prevention: How Tongue Hygiene Helps Maintain Balance of Microbiota and Overall Health in Pediatric Patients.Children (Basel). 2024 Jul 3;11(7):816. doi: 10.3390/children11070816. Children (Basel). 2024. PMID: 39062265 Free PMC article. Review.
-
Prevalence and associated factors of self-reported oral health problems among adults in the Fanteakwa districts in Ghana.BMC Oral Health. 2025 Jan 11;25(1):57. doi: 10.1186/s12903-024-05405-0. BMC Oral Health. 2025. PMID: 39799286 Free PMC article.
-
Tooth decay prevention and neurodevelopmental disorder risk following childhood fluoride exposure.BMC Pediatr. 2025 Apr 2;25(1):265. doi: 10.1186/s12887-025-05601-z. BMC Pediatr. 2025. PMID: 40170137 Free PMC article.
-
Racial Disparities in Quality of Dental Care Among Publicly Insured Children.Med Care. 2025 Sep 1;63(9):646-655. doi: 10.1097/MLR.0000000000002184. Epub 2025 Jul 7. Med Care. 2025. PMID: 40730339 Free PMC article.
References
-
- US Department of Health and Human Services . Oral health in America: a report of the Surgeon General. Accessed May 6, 2019. https://www.nidcr.nih.gov/research/data-statistics/surgeon-general
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
