

Acute kidney injury biomarkers and hydration assessments following prolonged mild hypohydration in healthy young adults
- PMID: 37318992
- PMCID: PMC10396285
- DOI: 10.1152/ajprenal.00086.2023
Acute kidney injury biomarkers and hydration assessments following prolonged mild hypohydration in healthy young adults
Abstract
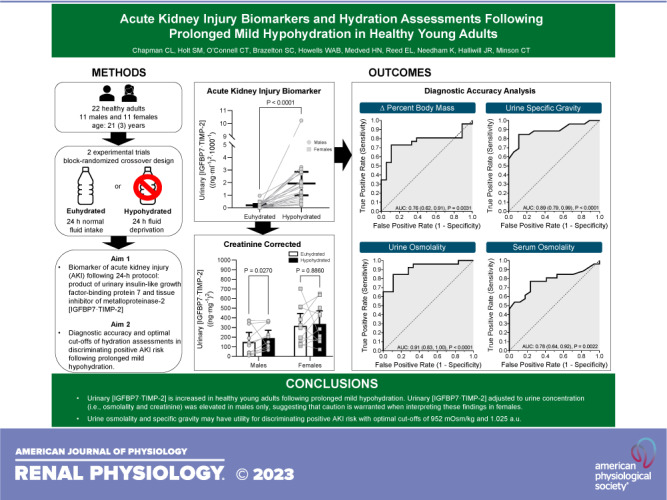
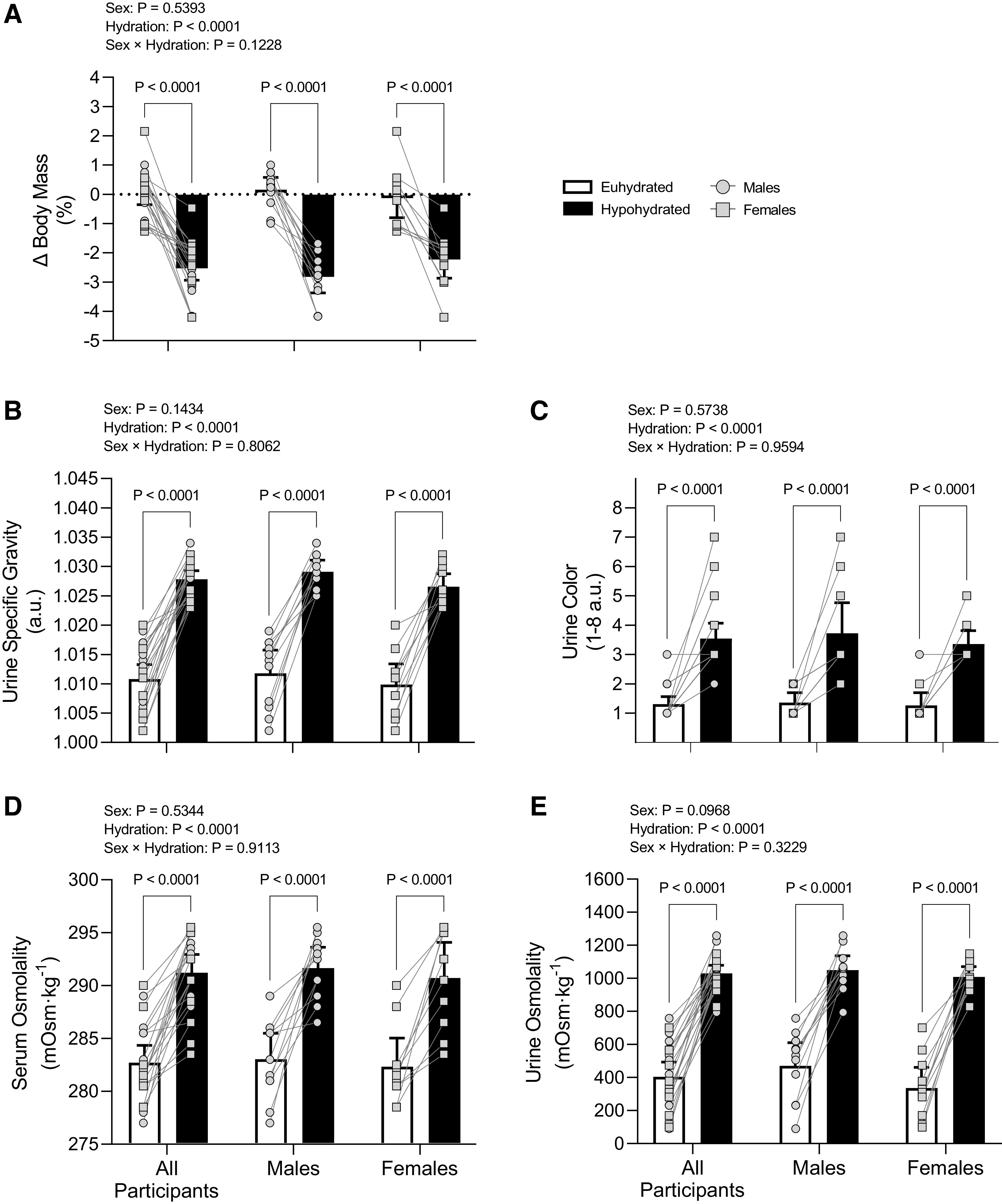
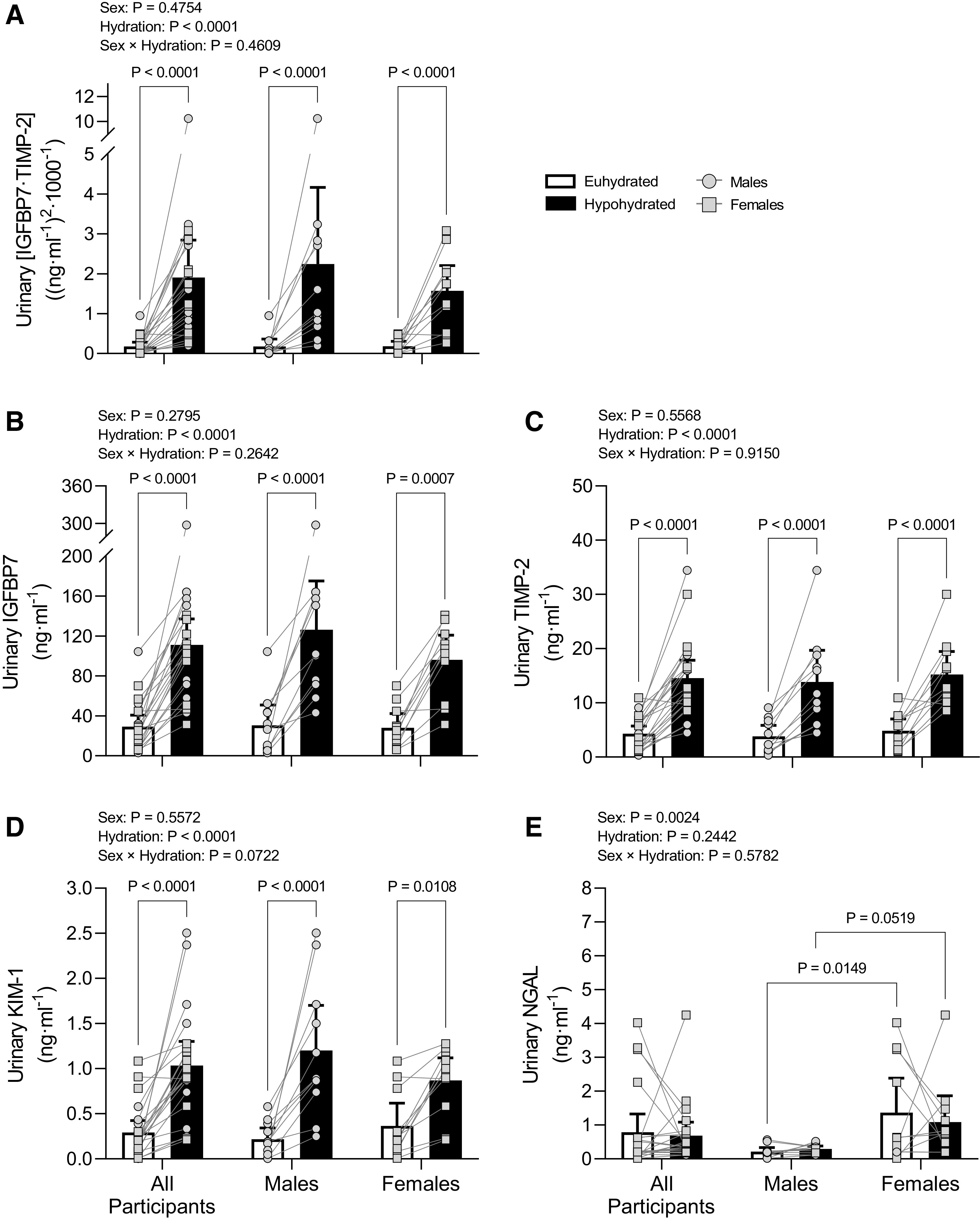
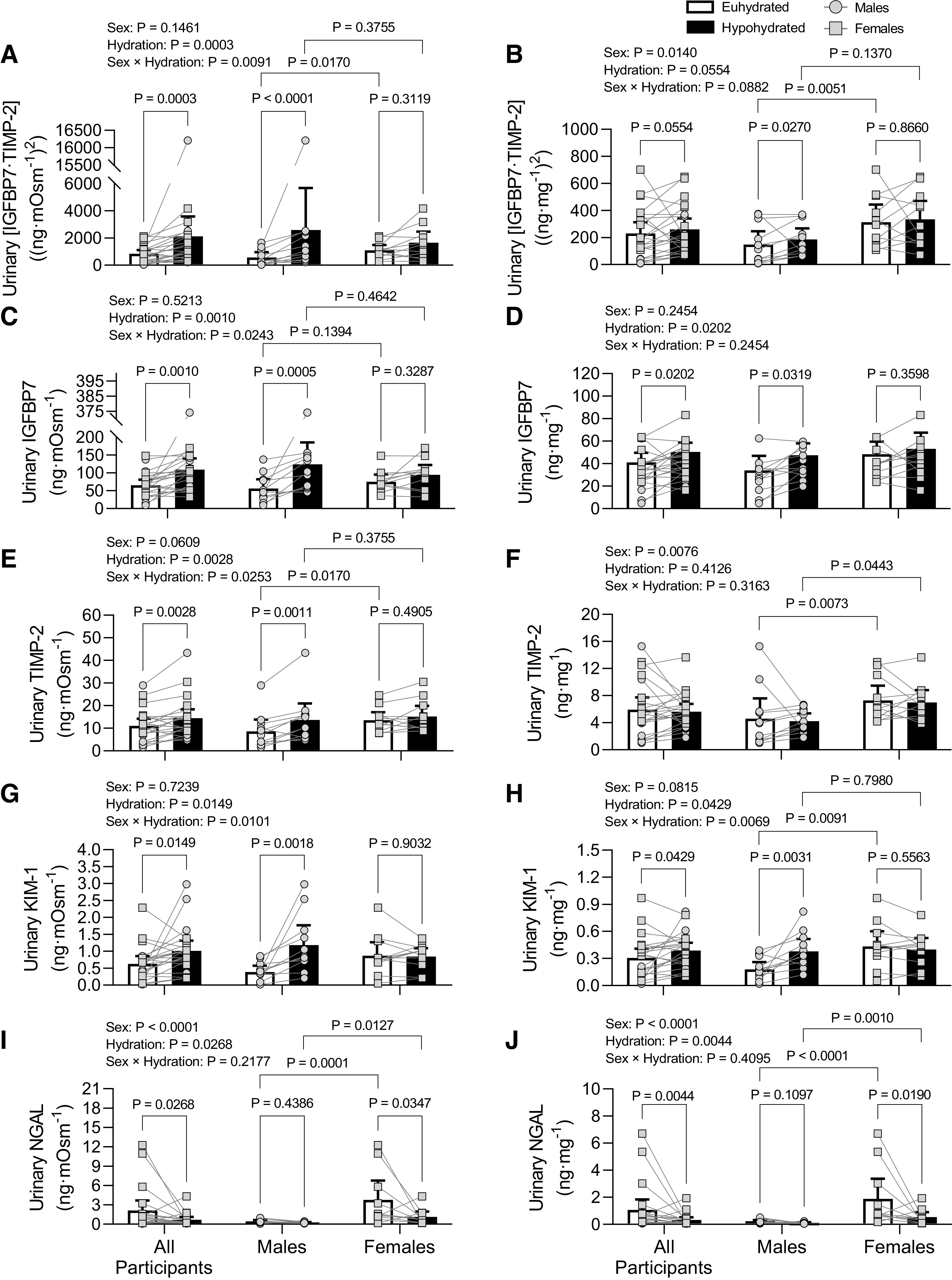
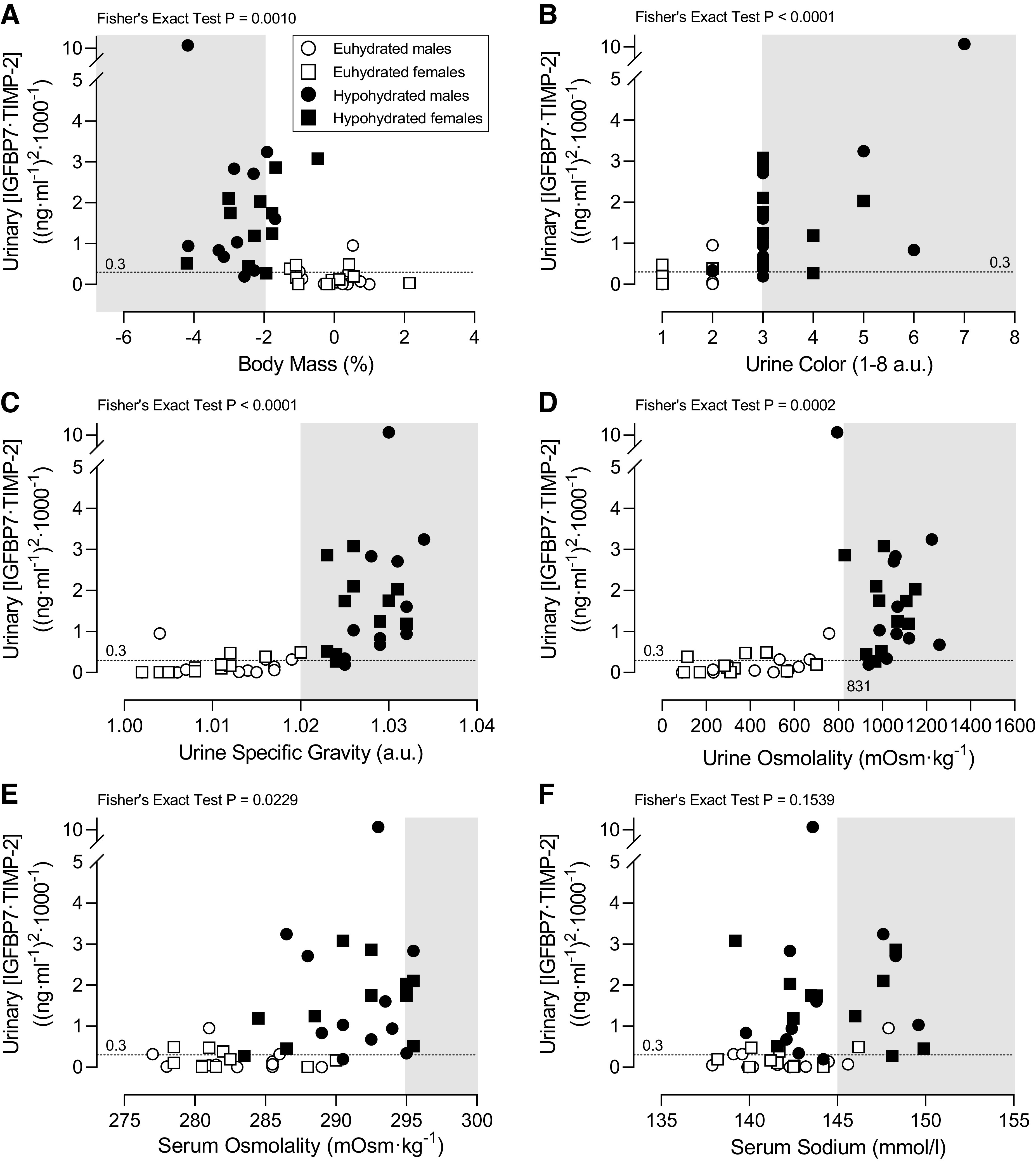
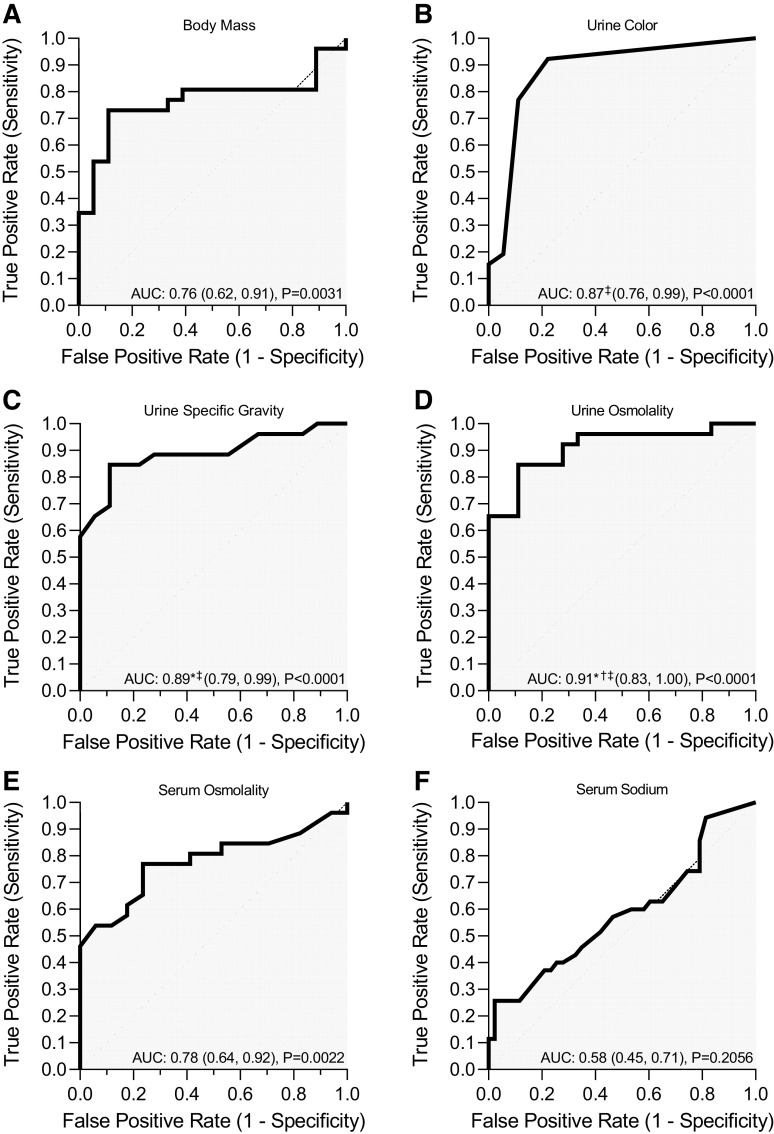
The high prevalence of inadequate hydration (e.g., hypohydration and underhydration) is concerning given that extreme heat increases excess hospitalizations for fluid/electrolyte disorders and acute kidney injury (AKI). Inadequate hydration may also be related to renal and cardiometabolic disease development. This study tested the hypothesis that prolonged mild hypohydration increases the urinary AKI biomarker product of insulin-like growth factor-binding protein 7 and tissue inhibitor of metalloproteinase-2 ([IGFBP7·TIMP-2]) compared with euhydration. In addition, we determined the diagnostic accuracy and optimal cutoffs of hydration assessments for discriminating positive AKI risk ([IGFBP·TIMP-2] >0.3 (ng/mL)2/1,000). In a block-randomized crossover design, 22 healthy young adults (11 females and 11 males) completed 24 h of fluid deprivation (hypohydrated group) or 24 h of normal fluid consumption (euhydrated group) separated by ≥72 h. Urinary [IGFBP7·TIMP-2] and other AKI biomarkers were measured following the 24-h protocols. Diagnostic accuracy was assessed via receiver operating characteristic curve analysis. Urinary [IGFBP7·TIMP-2] [1.9 (95% confidence interval: 1.0-2.8) vs. 0.2 (95% confidence interval: 0.1-0.3) (ng/mL)2/1,000, P = 0.0011] was markedly increased in hypohydrated versus euhydrated groups. Urine osmolality (area under the curve: 0.91, P < 0.0001) and urine specific gravity (area under the curve: 0.89, P < 0.0001) had the highest overall performance for discriminating positive AKI risk. Optimal cutoffs with a positive likelihood ratio of 11.8 for both urine osmolality and specific gravity were 952 mosmol/kgH2O and 1.025 arbitrary units. In conclusion, prolonged mild hypohydration increased urinary [IGFBP7·TIMP-2] in males and females. Urinary [IGFBP7·TIMP-2] corrected to urine concentration was elevated in males only. Urine osmolality and urine specific gravity may have clinical utility for discriminating positive AKI risk following prolonged mild hypohydration.NEW & NOTEWORTHY This study found that prolonged mild hypohydration in healthy young adults increased the Food and Drug Administration approved acute kidney injury (AKI) biomarker urinary insulin-like growth factor-binding protein 7 and tissue inhibitor of metalloproteinase-2 [IGFBP7·TIMP-2]. Urine osmolality and specific gravity demonstrated an excellent ability to discriminate positive AKI risk. These findings emphasize the importance of hydration in protecting renal health and lend early support for hydration assessment as an accessible tool to assess AKI risk.
Keywords: NephroCheck; dehydration; heat wave; kidney injury molecule-1; neutrophil gelatinase-associated lipocalin.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
Similar articles
-
Association of Renal Stress/Damage and Filtration Biomarkers with Subsequent AKI during Hospitalization among Patients Presenting to the Emergency Department.Clin J Am Soc Nephrol. 2016 Jun 6;11(6):938-946. doi: 10.2215/CJN.10551015. Epub 2016 Mar 29. Clin J Am Soc Nephrol. 2016. PMID: 27026519 Free PMC article.
-
Urinary tissue inhibitor of metalloproteinase-2 and insulin-like growth factor-binding protein 7 as biomarkers of patients with established acute kidney injury.Korean J Intern Med. 2020 May;35(3):662-671. doi: 10.3904/kjim.2018.266. Epub 2019 Dec 23. Korean J Intern Med. 2020. PMID: 31856559 Free PMC article.
-
Urinary TIMP-2 and IGFBP7 as early biomarkers of acute kidney injury and renal recovery following cardiac surgery.PLoS One. 2014 Mar 27;9(3):e93460. doi: 10.1371/journal.pone.0093460. eCollection 2014. PLoS One. 2014. PMID: 24675717 Free PMC article. Clinical Trial.
-
Current understanding and future directions in the application of TIMP-2 and IGFBP7 in AKI clinical practice.Clin Chem Lab Med. 2019 Apr 24;57(5):567-576. doi: 10.1515/cclm-2018-0776. Clin Chem Lab Med. 2019. PMID: 30179848 Review.
-
The diagnostic accuracy of urinary [TIMP-2]·[IGFBP7] for acute kidney injury in adults: A PRISMA-compliant meta-analysis.Medicine (Baltimore). 2017 Jul;96(27):e7484. doi: 10.1097/MD.0000000000007484. Medicine (Baltimore). 2017. PMID: 28682920 Free PMC article. Review.
Cited by
-
Occupational cold stress and rewarming alters skin temperature thresholds for manual dexterity decrements: An exploratory study.Physiol Rep. 2025 May;13(9):e70342. doi: 10.14814/phy2.70342. Physiol Rep. 2025. PMID: 40343410 Free PMC article.
-
Shifting focus: Time to look beyond the classic physiological adaptations associated with human heat acclimation.Exp Physiol. 2024 Mar;109(3):335-349. doi: 10.1113/EP091207. Epub 2023 Oct 26. Exp Physiol. 2024. PMID: 37885125 Free PMC article. Review.
-
The multifaceted role of insulin-like growth factor binding protein 7.Front Cell Dev Biol. 2024 Jul 16;12:1420862. doi: 10.3389/fcell.2024.1420862. eCollection 2024. Front Cell Dev Biol. 2024. PMID: 39081862 Free PMC article. Review.
-
Acute exposure to carbon monoxide inhalation and/or hot water immersion transiently increases erythropoietin in females but not in males.Exp Physiol. 2024 Oct;109(10):1782-1795. doi: 10.1113/EP091923. Epub 2024 Aug 15. Exp Physiol. 2024. PMID: 39143855 Free PMC article. Clinical Trial.
-
Sex differences in biomarkers of end-organ damage following exertional heat stroke in humans.J Appl Physiol (1985). 2024 Nov 1;137(5):1434-1445. doi: 10.1152/japplphysiol.00463.2024. Epub 2024 Sep 19. J Appl Physiol (1985). 2024. PMID: 39298615 Free PMC article.
References
-
- Schramm PJ, Vaidyanathan A, Radhakrishnan L, Gates A, Hartnett K, Breysse P. Heat-related emergency department visits during the northwestern heat wave—United States, June 2021. MMWR Morb Mortal Wkly Rep 70: 1020–1021, 2021. [Erratum in MMWR Morb Mortal Wkly Rep 70: 1103, 2021]. doi:10.15585/mmwr.mm7029e1. - DOI - PMC - PubMed
-
- Lin H, Mo R, Vitart F. The 2021 western North American heatwave and its subseasonal predictions. Geophys Res Lett 49: e2021GL097036, 2022. doi:10.1029/2021GL097036. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous