

Focused ultrasound thalamotomy for tremor treatment impacts the cerebello-thalamo-cortical network
- PMID: 37322044
- PMCID: PMC10272231
- DOI: 10.1038/s41531-023-00543-8
Focused ultrasound thalamotomy for tremor treatment impacts the cerebello-thalamo-cortical network
Abstract
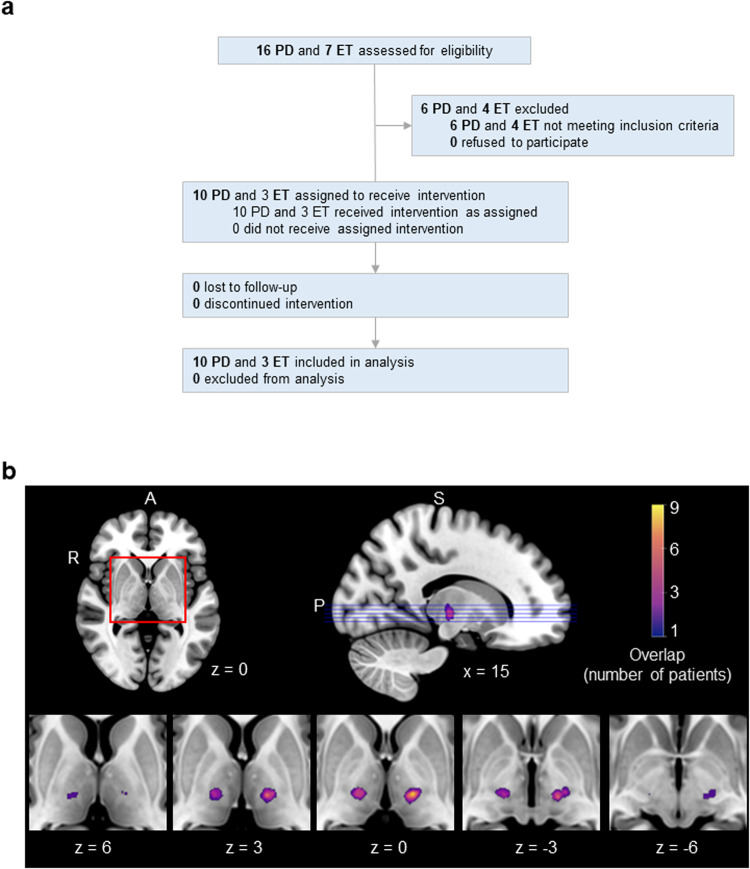
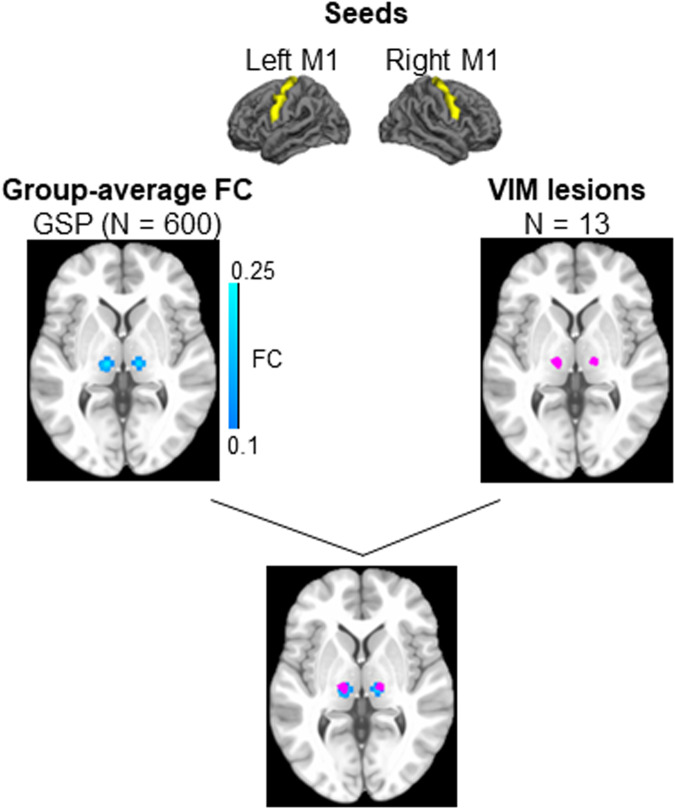
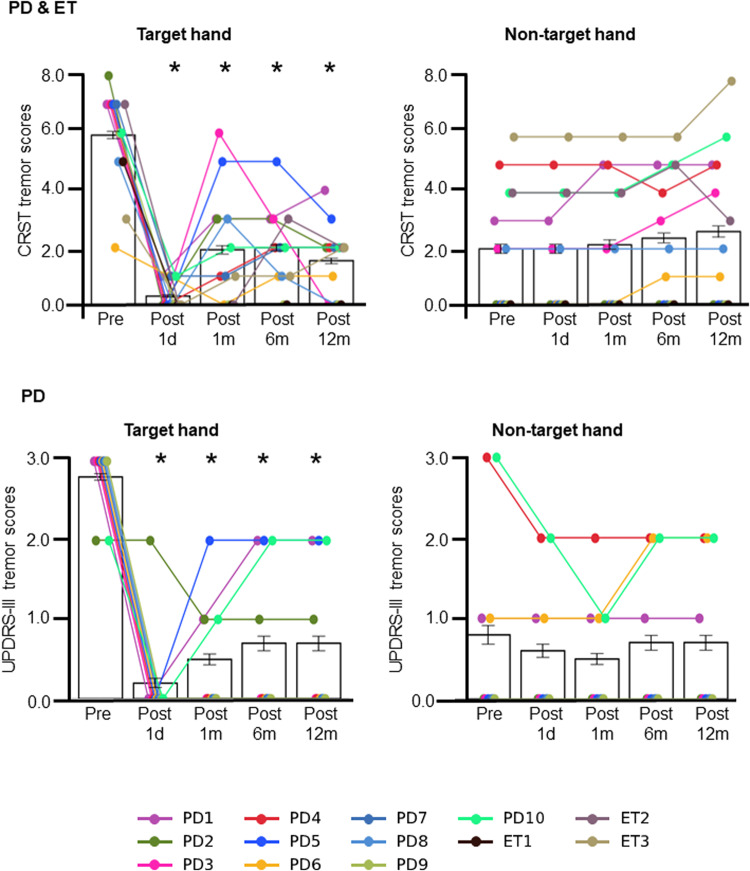
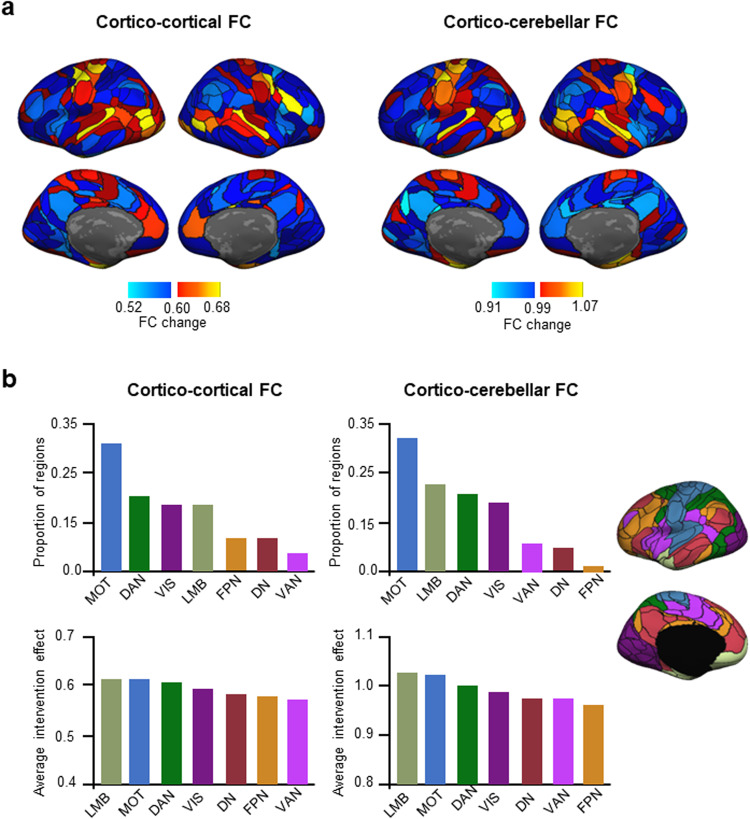
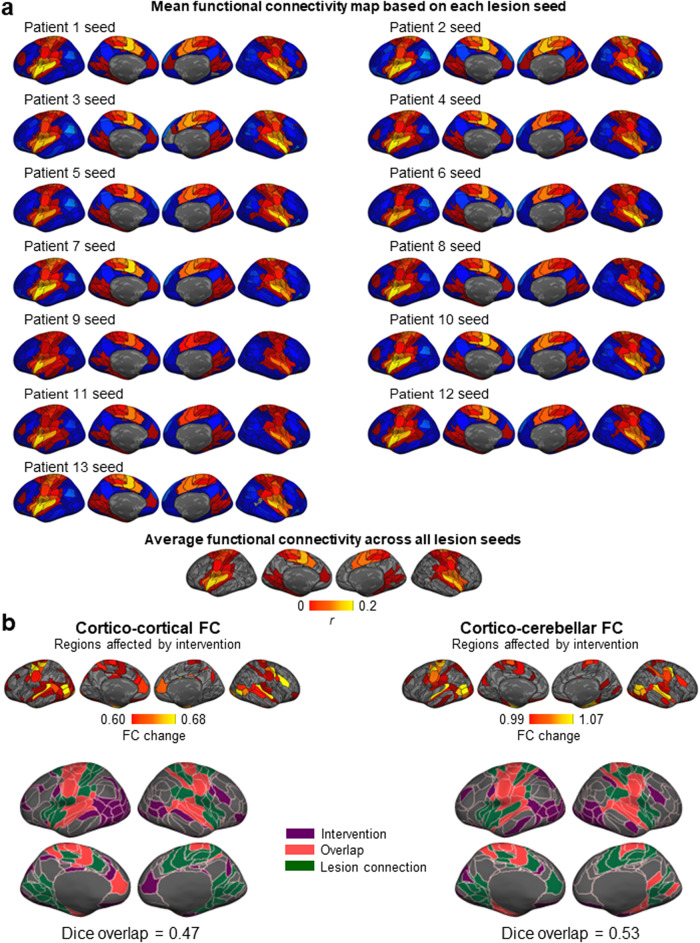
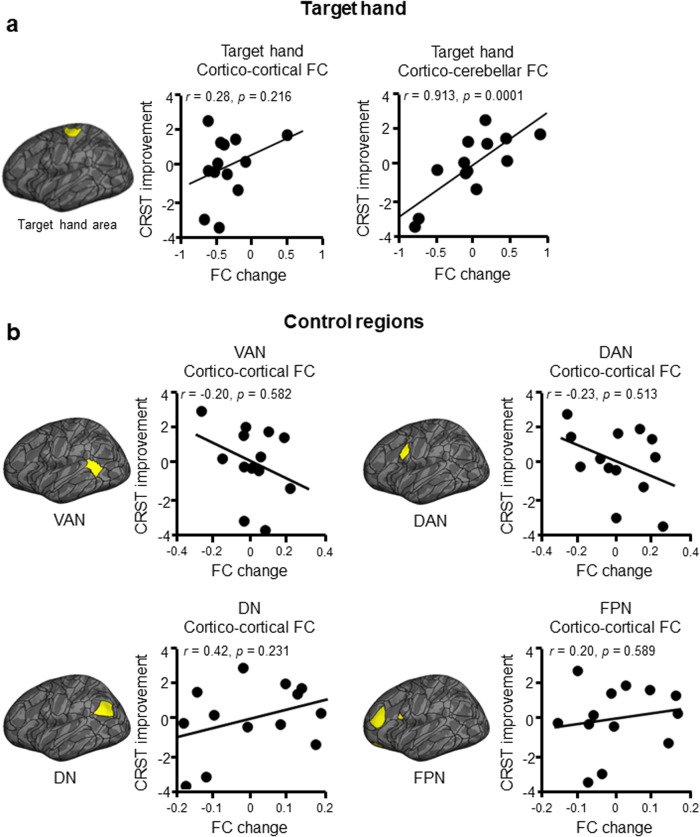
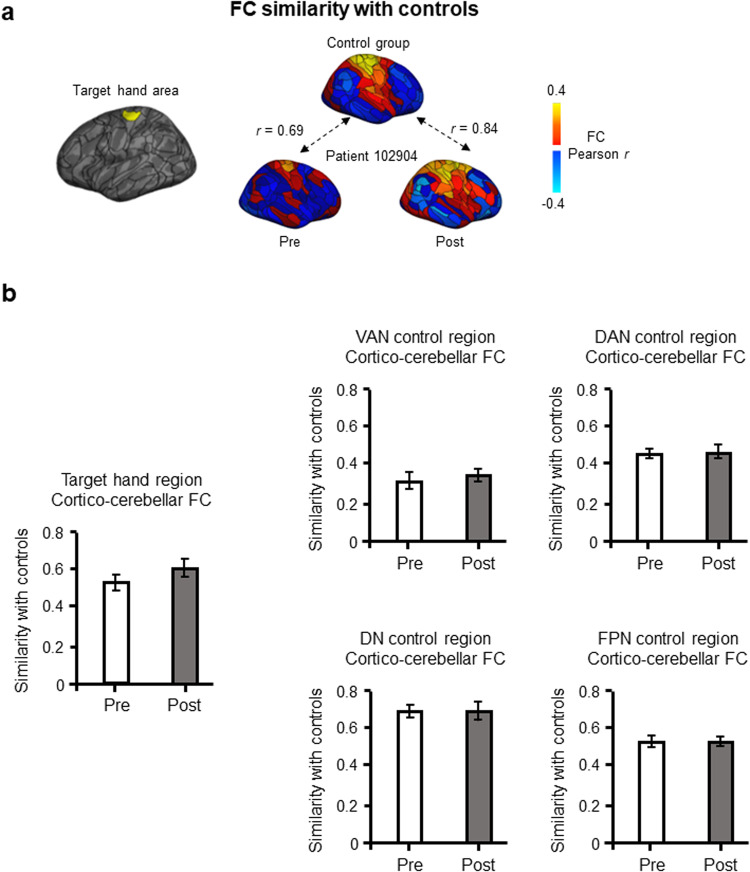
High-intensity Magnetic Resonance-guided Focused Ultrasound (MRgFUS) is a recent, non-invasive line of treatment for medication-resistant tremor. We used MRgFUS to produce small lesions in the thalamic ventral intermediate nucleus (VIM), an important node in the cerebello-thalamo-cortical tremor network, in 13 patients with tremor-dominant Parkinson's disease or essential tremor. Significant tremor alleviation in the target hand ensued (t(12) = 7.21, p < 0.001, two-tailed), which was strongly associated with the functional reorganization of the brain's hand region with the cerebellum (r = 0.91, p < 0.001, one-tailed). This reorganization potentially reflected a process of normalization, as there was a trend of increase in similarity between the hand cerebellar connectivity of the patients and that of a matched, healthy control group (n = 48) after treatment. Control regions in the ventral attention, dorsal attention, default, and frontoparietal networks, in comparison, exhibited no association with tremor alleviation and no normalization. More broadly, changes in functional connectivity were observed in regions belonging to the motor, limbic, visual, and dorsal attention networks, largely overlapping with regions connected to the lesion targets. Our results indicate that MRgFUS is a highly efficient treatment for tremor, and that lesioning the VIM may result in the reorganization of the cerebello-thalamo-cortical tremor network.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
MR-guided focused ultrasound thalamotomy modulates cerebello-thalamo-cortical tremor network in essential tremor patients.Front Neurol. 2025 Apr 22;16:1526501. doi: 10.3389/fneur.2025.1526501. eCollection 2025. Front Neurol. 2025. PMID: 40330248 Free PMC article.
-
Magnetic resonance-guided focused ultrasound thalamotomy restored distinctive resting-state networks in patients with essential tremor.J Neurosurg. 2022 Jul 8;138(2):306-317. doi: 10.3171/2022.5.JNS22411. Print 2023 Feb 1. J Neurosurg. 2022. PMID: 35901706
-
Magnetic resonance-guided focused ultrasound thalamotomy for tremor: a report of 30 Parkinson's disease and essential tremor cases.J Neurosurg. 2018 Jan;128(1):202-210. doi: 10.3171/2016.10.JNS16758. Epub 2017 Feb 24. J Neurosurg. 2018. PMID: 28298022
-
An experience-based review of HIFU in functional interventional neuroradiology: transcranial MRgFUS thalamotomy for treatment of tremor.Radiol Med. 2020 Sep;125(9):877-886. doi: 10.1007/s11547-020-01186-y. Epub 2020 Apr 7. Radiol Med. 2020. PMID: 32266693 Review.
-
Magnetic resonance-guided focused ultrasound for the treatment of tremor.Expert Rev Neurother. 2022 Oct;22(10):849-861. doi: 10.1080/14737175.2022.2147826. Epub 2022 Dec 5. Expert Rev Neurother. 2022. PMID: 36469578 Review.
Cited by
-
Magnetic Resonance-Guided Focused Ultrasound Thalamotomy in a Prospective Cohort of 52 Patients with Parkinson's Disease: A Possible Critical Role of Age and Lesion Volume for Predicting Tremor Relapse.Mov Disord. 2025 Mar;40(3):478-489. doi: 10.1002/mds.30093. Epub 2025 Jan 18. Mov Disord. 2025. PMID: 39825750 Free PMC article.
-
Efficacy and safety of magnetic resonance-guided focused ultrasound for Parkinson's disease: a systematic review and meta-analysis.Front Neurol. 2023 Dec 7;14:1301240. doi: 10.3389/fneur.2023.1301240. eCollection 2023. Front Neurol. 2023. PMID: 38146437 Free PMC article.
-
MR-guided focused ultrasound thalamotomy in a patient with thrombocytopenia: illustrative case.J Neurosurg Case Lessons. 2025 Jul 21;10(3):CASE2525. doi: 10.3171/CASE2525. Print 2025 Jul 21. J Neurosurg Case Lessons. 2025. PMID: 40690800 Free PMC article.
-
Individualized functional connectivity markers associated with motor and mood symptoms of Parkinson's disease.bioRxiv [Preprint]. 2024 Feb 2:2024.01.31.578238. doi: 10.1101/2024.01.31.578238. bioRxiv. 2024. PMID: 38352322 Free PMC article. Preprint.
-
Early re-emerging tremor after MRgFUS thalamotomy: case-control analysis of procedural and imaging features.Front Neurol. 2024 Jun 6;15:1356613. doi: 10.3389/fneur.2024.1356613. eCollection 2024. Front Neurol. 2024. PMID: 38903176 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
