

Attributed causes of excess mortality during the COVID-19 pandemic in a south Indian city
- PMID: 37322091
- PMCID: PMC10272147
- DOI: 10.1038/s41467-023-39322-7
Attributed causes of excess mortality during the COVID-19 pandemic in a south Indian city
Abstract
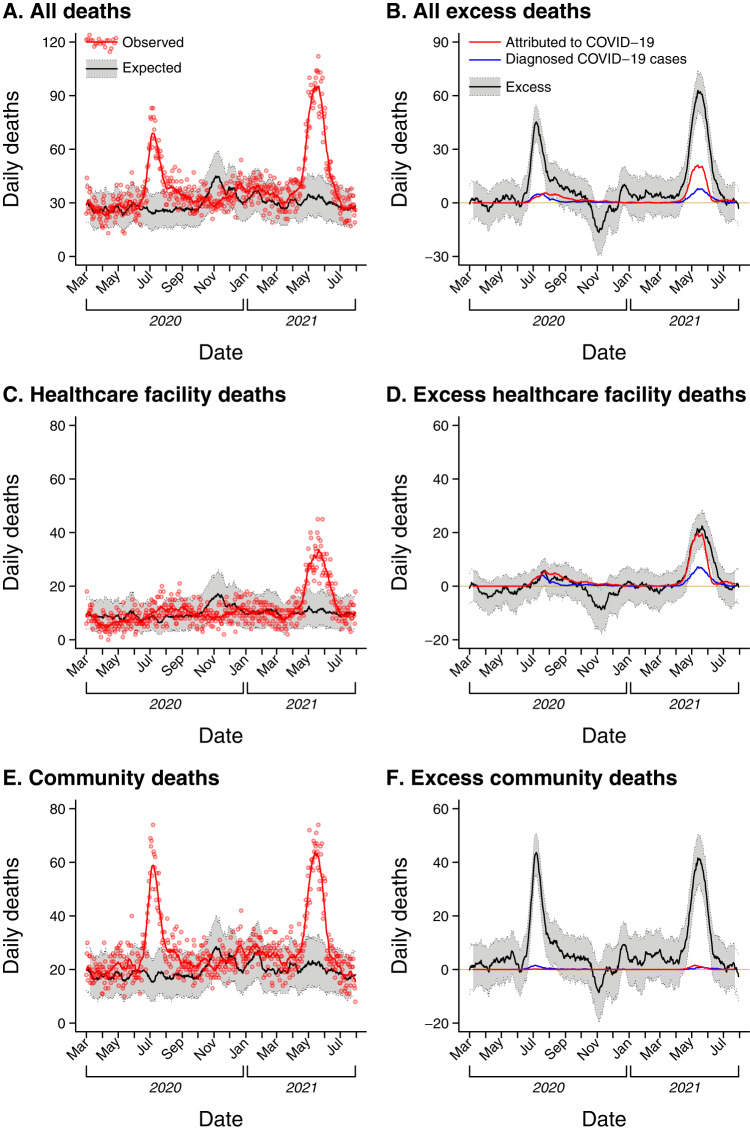
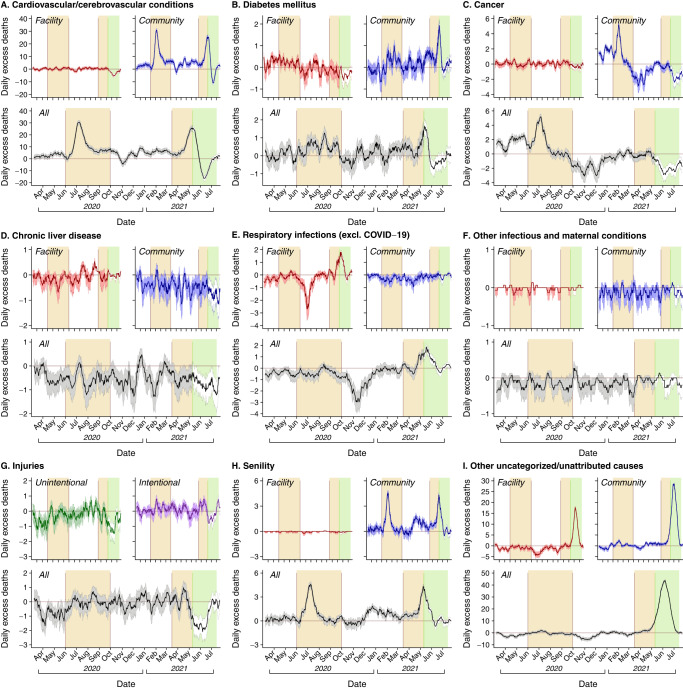
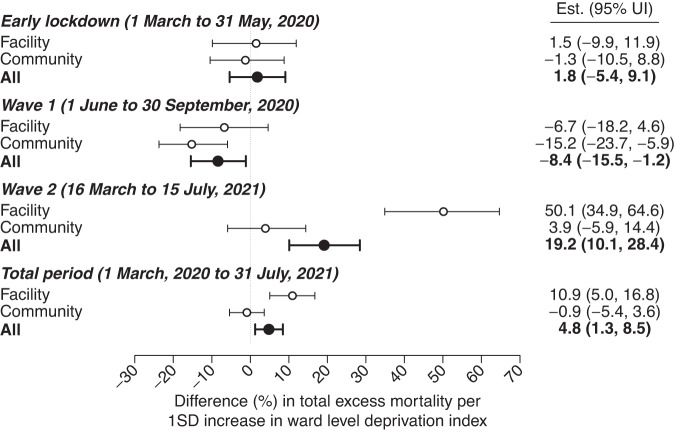
Globally, excess deaths during 2020-21 outnumbered documented COVID-19 deaths by 9.5 million, primarily driven by deaths in low- and middle-income countries (LMICs) with limited vital surveillance. Here we unravel the contributions of probable COVID-19 deaths from other changes in mortality related to pandemic control measures using medically-certified death registrations from Madurai, India-an urban center with well-functioning vital surveillance. Between March, 2020 and July, 2021, all-cause deaths in Madurai exceeded expected levels by 30% (95% confidence interval: 27-33%). Although driven by deaths attributed to cardiovascular or cerebrovascular conditions, diabetes, senility, and other uncategorized causes, increases in these attributions were restricted to medically-unsupervised deaths, and aligned with surges in confirmed or attributed COVID-19 mortality, likely reflecting mortality among unconfirmed COVID-19 cases. Implementation of lockdown measures was associated with a 7% (0-13%) reduction in all-cause mortality, driven by reductions in deaths attributed to injuries, infectious diseases and maternal conditions, and cirrhosis and other liver conditions, respectively, but offset by a doubling in cancer deaths. Our findings help to account for gaps between documented COVID-19 mortality and excess all-cause mortality during the pandemic in an LMIC setting.
© 2023. The Author(s).
Conflict of interest statement
J.A.L. discloses receipt of grants and honoraria from Pfizer unrelated to this research. The remaining authors declare no competing interest.
Figures
References
-
- World Health Organization. Global excess deaths associated with COVID-19, January 2020 - December 2021. Available from: https://www.who.int/data/stories/global-excess-deaths-associated-with-co.... (2023).
-
- Mishra V, et al. Drought and famine in India, 1870–2016. Geophys. Res. Lett. 2019;46:2075–2083. doi: 10.1029/2018GL081477. - DOI
