

The NCI-MATCH trial: lessons for precision oncology
- PMID: 37322121
- PMCID: PMC10612141
- DOI: 10.1038/s41591-023-02379-4
The NCI-MATCH trial: lessons for precision oncology
Abstract
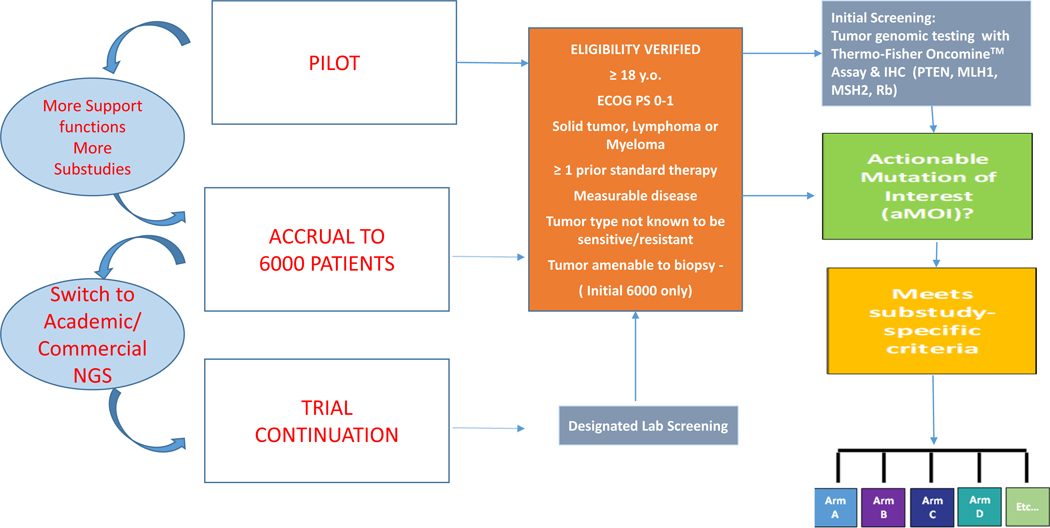
The NCI-MATCH (Molecular Analysis for Therapy Choice) trial ( NCT02465060 ) was launched in 2015 as a genomically driven, signal-seeking precision medicine platform trial-largely for patients with treatment-refractory, malignant solid tumors. Having completed in 2023, it remains one of the largest tumor-agnostic, precision oncology trials undertaken to date. Nearly 6,000 patients underwent screening and molecular testing, with a total of 1,593 patients (inclusive of continued accrual from standard next-generation sequencing) being assigned to one of 38 substudies. Each substudy was a phase 2 trial of a therapy matched to a genomic alteration, with a primary endpoint of objective tumor response by RECIST criteria. In this Perspective, we summarize the outcomes of the initial 27 substudies in NCI-MATCH, which met its signal-seeking objective with 7/27 positive substudies (25.9%). We discuss key aspects of the design and operational conduct of the trial, highlighting important lessons for future precision medicine studies.
© 2023. Springer Nature America, Inc.
Figures
References
-
- Kopetz S, Desai J, Chan E, Hecht JR, O’Dwyer PJ, Maru D, Morris V, Janku F, Dasari A, Chung W, Issa JP, Gibbs P, James B, Powis G, Nolop KB, Bhattacharya S, Saltz L. Phase II Pilot Study of Vemurafenib in Patients With Metastatic BRAF-Mutated Colorectal Cancer. J Clin Oncol. 2015. Dec 1;33(34):4032–8. - PMC - PubMed
-
- Wheeler DA, Srinivasan M, Egholm M, Shen Y, Chen L, McGuire A, He W, Chen YJ, Makhijani V, Roth GT, Gomes X, Tartaro K, Niazi F, Turcotte CL, Irzyk GP, Lupski JR, Chinault C, Song XZ, Liu Y, Yuan Y, Nazareth L, Qin X, Muzny DM, Margulies M, Weinstock GM, Gibbs RA, Rothberg JM. The complete genome of an individual by massively parallel DNA sequencing. Nature. 2008. Apr 17;452(7189):872–6. doi: 10.1038/nature06884. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
