

Long-term Effectiveness and Safety of Upadacitinib for Atopic Dermatitis in a Real-world Setting: An Interim Analysis Through 48 Weeks of Observation
- PMID: 37322324
- PMCID: PMC10570196
- DOI: 10.1007/s40257-023-00798-0
Long-term Effectiveness and Safety of Upadacitinib for Atopic Dermatitis in a Real-world Setting: An Interim Analysis Through 48 Weeks of Observation
Erratum in
-
Correction to: Long-term Effectiveness and Safety of Upadacitinib for Atopic Dermatitis in a Real-world Setting: An Interim Analysis Through 48 Weeks of Observation.Am J Clin Dermatol. 2023 Nov;24(6):963-964. doi: 10.1007/s40257-023-00813-4. Epub 2023 Aug 19. Am J Clin Dermatol. 2023. PMID: 37597128 Free PMC article. No abstract available.
Abstract
Background: Janus kinase (JAK) inhibitors, including upadacitinib, have been recently approved for the treatment of moderate-severe atopic dermatitis (AD) and real-world data on upadacitinib effectiveness and safety are limited. This interim analysis aimed to assess effectiveness and safety of upadacitinib throughout 48 weeks of observation in a real-world adult AD population.
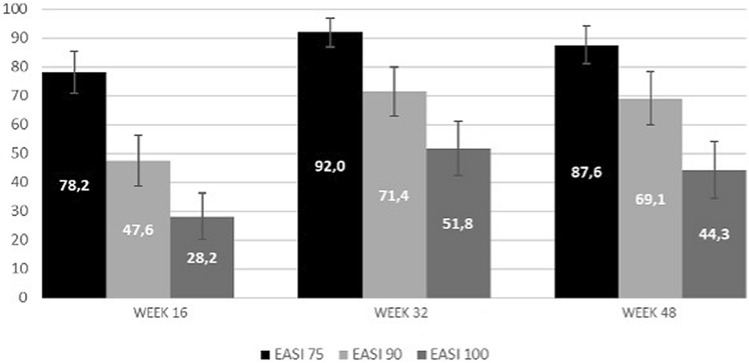
Methods: This prospective study collected data on adult patients affected by moderate-to-severe AD and treated with upadacitinib at the dosage of either 15 mg or 30 mg daily based on the physician decision. Upadacitinib was prescribed in the context of a national compassionate use programme. In this interim analysis, within patient comparisons of continuous scores of different scales (namely Eczema Area and Severity Index [EASI], body surface area [BSA], Dermatology Life Quality Index [DLQI], Patient Oriented Eczema Measure [POEM], Numeric Rating Scale [NRS] subtests) were performed. The percentage of patients achieving EASI 75, EASI 90 and EASI 100 at Week 16, 32 and 48 was also evaluated.
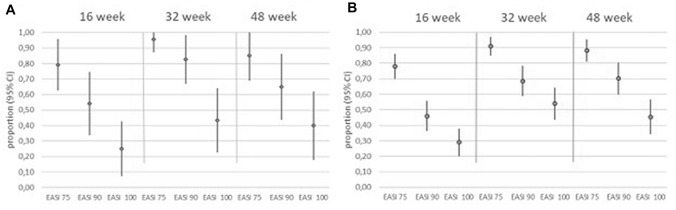
Results: One hundred and forty-six patients were included in the analysis. Upadacitinib 15 mg or 30 mg daily was prescribed as monotherapy in most cases (127/146, 87.0%). Upadacitinib was initially prescribed at the dosage of 30 mg daily in 118 of 146 (80.8%) patients and 15 mg daily in 28/146 (19.2%) patients. A significant improvement in the clinical signs and symptoms of AD was detected by Week 16 and throughout the study period. EASI 75, EASI 90 and EASI 100 responses were achieved by 87.6%, 69.1% and 44.3% at Week 48, associated with a sustained reduction in the mean values of all physician-reported (EASI and BSA) and patient-reported (Itch- Sleep- and Pain-NRS, DLQI, and POEM) disease severity outcomes, up to 48 weeks of treatment. Treatment response observed in 15 mg upadacitinib-treated patients was comparable with that detected in 30 mg upadacitinib-treated patients, revealing no statistical difference between the two patient sub-cohorts. Through the observation period, dose reduction or escalation was observed in 38/146 (26%) of treated cases. Overall, 26 of 146 (17.8%) patients experienced at least one adverse event (AE) during the treatment period. In total, 29 AEs were recorded and most of them were evaluated as mild to moderate, while in 4 cases the occurrence of AE led to drug discontinuation, for a total of 7/146 (4.8%) dropouts.
Conclusion: This study provides strong evidence of a sustained response obtained by upadacitinib in AD patients, who had failed to respond to conventional or biological systemic agents, through 48 weeks of observation. Upadacitinib was also demonstrated to be advantageous in terms of flexibility in dose reduction or escalation as upadacitinib dose was shaped on clinical needs that, in a real-world setting, might frequently change.
© 2023. The Author(s).
Conflict of interest statement
Alberto Maria Bertoldi has received honoraria for lectures for AbbVie and Sanofi. Andrea Chiricozzi has served as advisory board member and consultant and has received fees and speaker's honoraria or has participated in clinical trials for AbbVie, Almirall, Bristol Myers Squibb, Leo Pharma, Lilly, Janssen, Novartis, Pfizer and Sanofi Genzyme. Maria Concetta Fargnoli has served on advisory boards, received honoraria for lectures and/or research grants from AMGEN, Almirall, Abbvie, Boehringer-Ingelheim, BMS, Galderma, Kyowa Kyrin, Leo Pharma, Pierre Fabre, UCB, Lilly, Pfizer, Janssen, MSD, Novartis, Sanofi-Regeneron, Sunpharma. Silvia Ferrucci has been principal investigator in clinical trials for ABBVIE, Almirall, Galderma, Leo Pharma, Sanofi, Amgen, Novartis, Bayer and received honoraria for lectures for Novartis and Menarini. Giampiero Girolomoni has received personal fees from AbbVie, Abiogen, Almirall, Amgen, Biogen, Boehringer-Ingelheim, Bristol-Myers Squibb, Eli-Lilly, Leo Pharma, Merck Serono, Novartis, Pfizer, Samsung and Sanofi. Niccolò Gori served as advisory board member and received honoraria for lectures for AbbVie, Sanofi, and Leo-Pharma. Angelo Valerio Marzano reports consultancy/advisory boards disease-relevant honoraria from AbbVie, Boehringer-Ingelheim, Novartis, Pfizer, Sanofi and UCB. Michela Ortoncelli has served as advisory board member and/or consultant and has received fees and speaker's honoraria or has participated for clinical studies for AbbVie, Leo Pharma, and Sanofi Genzyme. Ketty Peris has served on advisory board, received honoraria for lectures and/or research grants for Abbvie, Almirall, Lilly, Galderma, Leo Pharma, Pierre Fabre, Novartis, Sanofi, Sun Pharma, Janssen. Simone Ribero has served as advisory board member and/or consultant and has received fees and speaker's honoraria or has participated for clinical studies for AbbVie, Almirall, Leo Pharma, Elli Lilly, Novartis, Pfizer and Sanofi Genzyme. Marco Romanelli has served as advisory board member and consultant and has received fees and speaker's honoraria or has participated in clinical trials for Abbvie Almirall, Bristol Myers Squibb, Leo Pharma, Lilly, Janssen Novartis, Sanofi Genzyme. The other authors have no competing interests to declare.
Figures
References
-
- de Bruin-Weller M, Thaçi D, Smith CH, et al. Dupilumab with concomitant topical corticosteroid treatment in adults with atopic dermatitis with an inadequate response or intolerance to ciclosporin A or when this treatment is medically inadvisable: a placebo-controlled, randomized phase III clinical trial (LIBERTY AD CAFÉ) Br J Dermatol. 2018;178:1083–1101. doi: 10.1111/bjd.16156. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
