

Clinical efficacy of bioactive restorative materials in controlling secondary caries: a systematic review and network meta-analysis
- PMID: 37322456
- PMCID: PMC10268411
- DOI: 10.1186/s12903-023-03110-y
Clinical efficacy of bioactive restorative materials in controlling secondary caries: a systematic review and network meta-analysis
Abstract
Background: This systematic review and network meta-analysis aimed to compare the clinical efficacy of bioactive and conventional restorative materials in controlling secondary caries (SC) and to provide a classification of these materials according to their effectiveness.
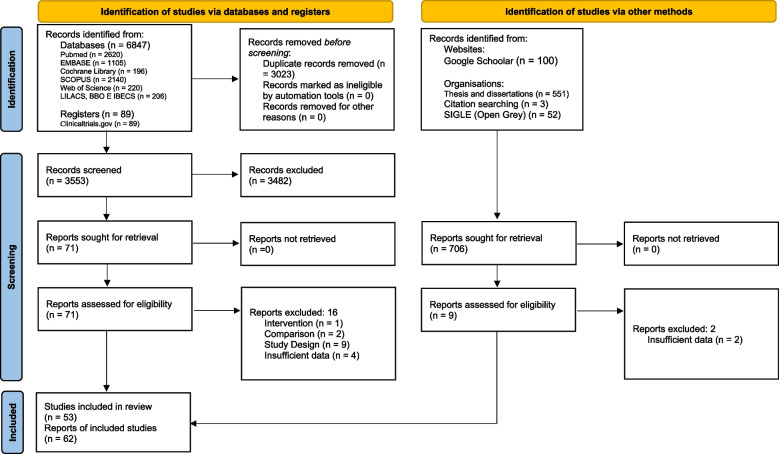
Methods: A search was performed in Pubmed, Web of Science, Embase, BBO, Lilacs, Cochrane Library, Scopus, IBECS and gray literature. Clinical trials were included, with no language or publication date limitations. Paired and network meta-analyses were performed with random-effects models, comparing treatments of interest and classifying them according to effectiveness in the permanent and deciduous dentition and at 1-year or 2/more years of follow-up. The risk of bias and certainty of evidence were evaluated.
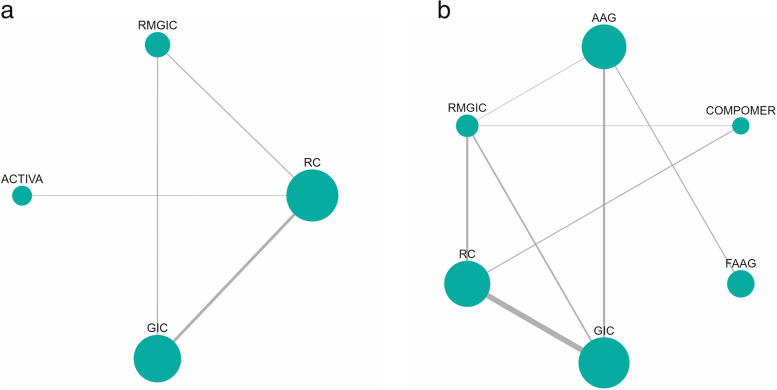
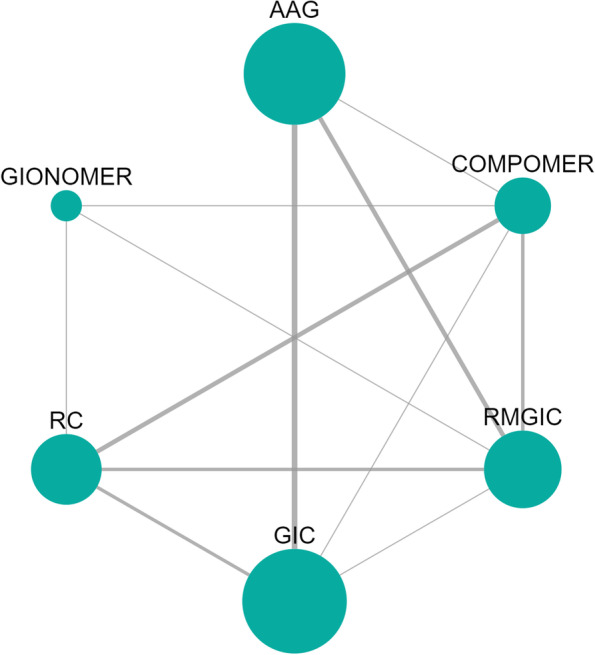
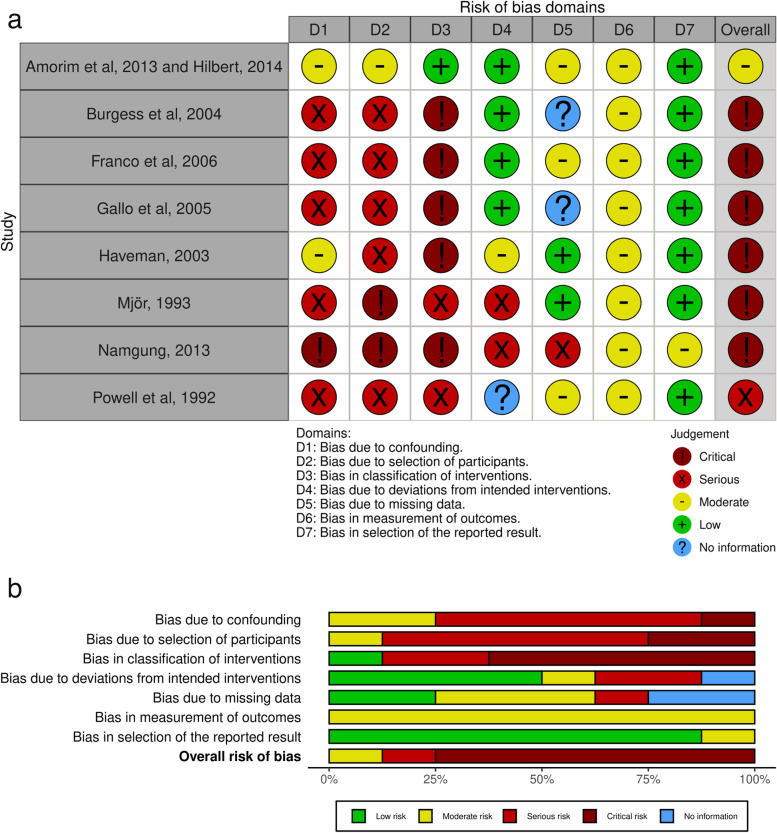
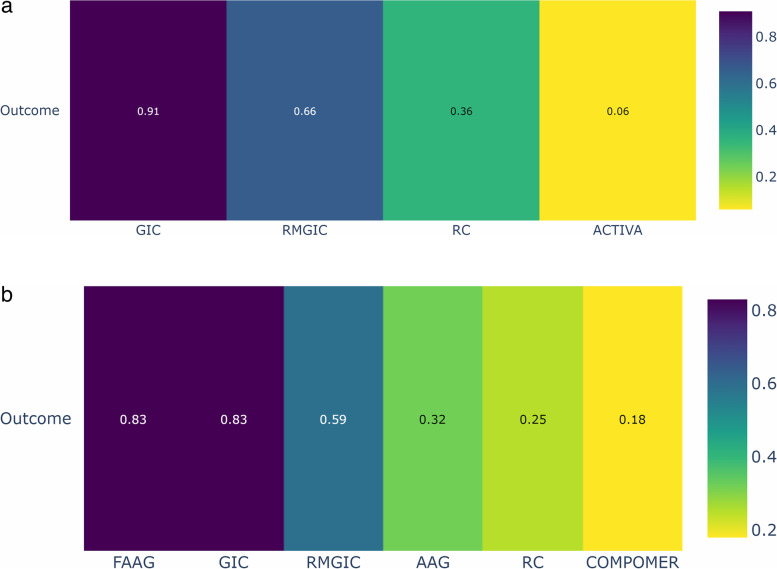
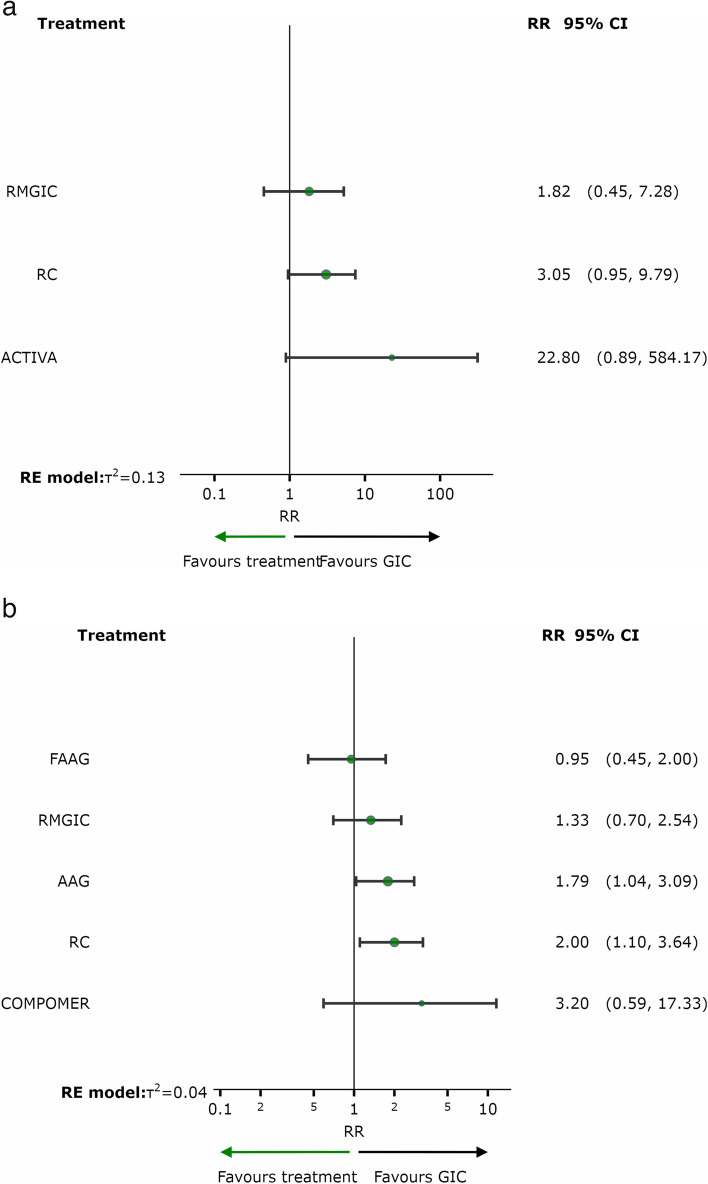
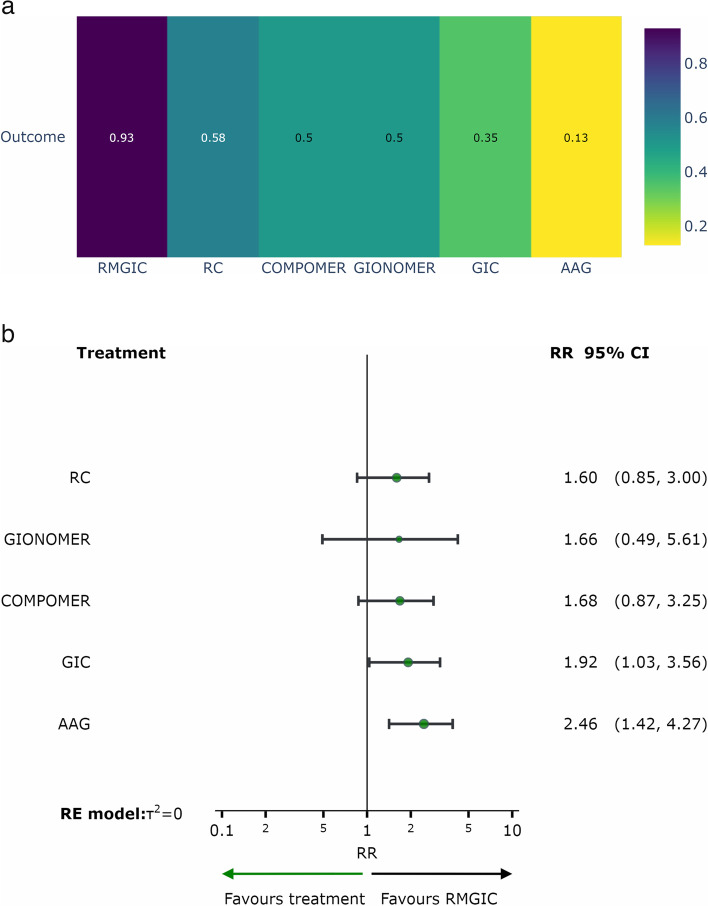
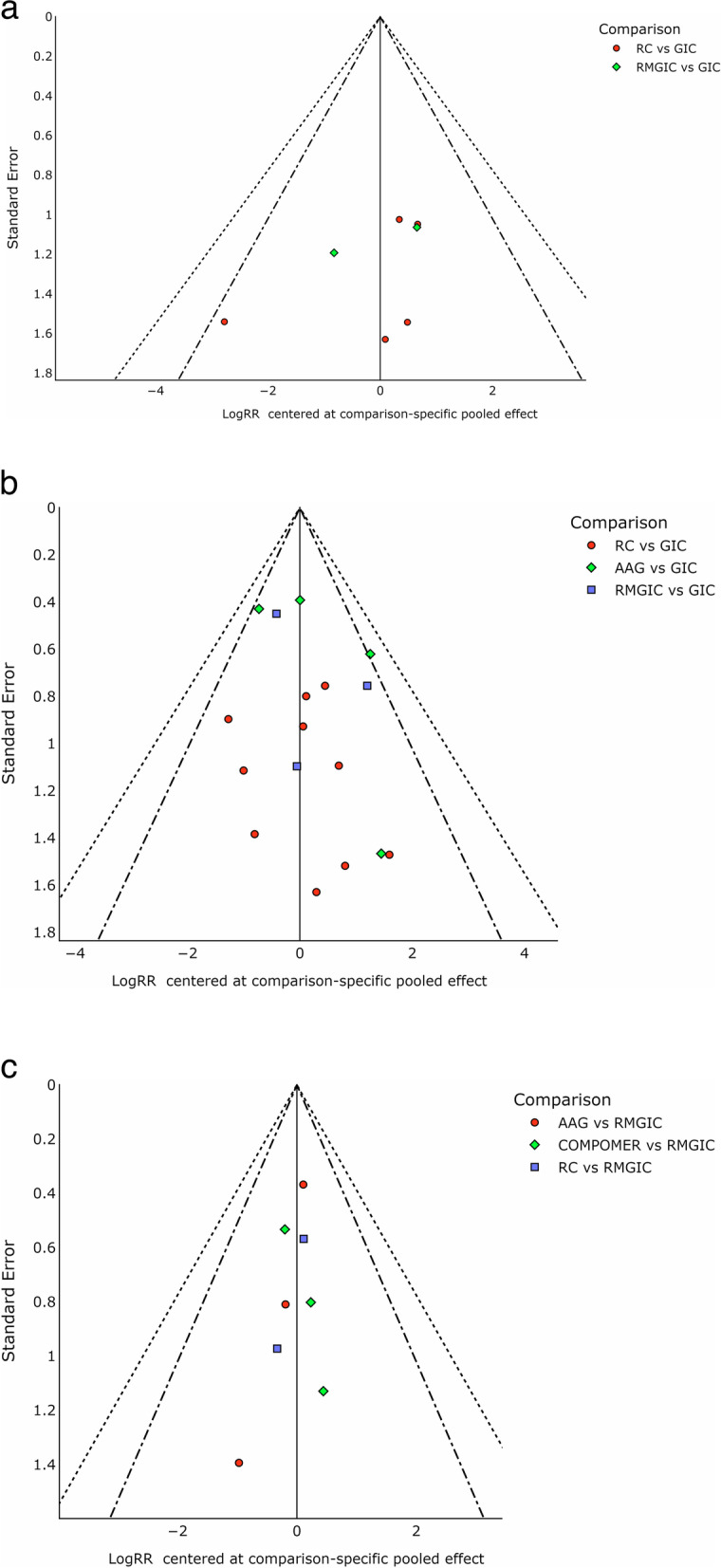
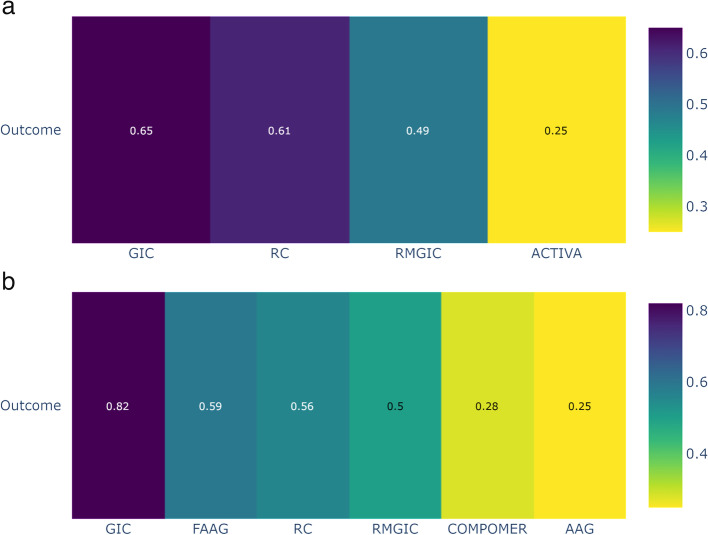
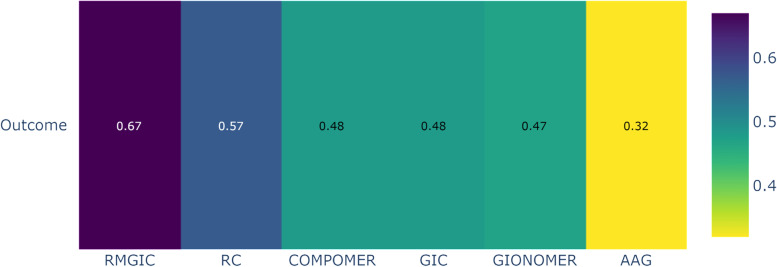
Results: Sixty-two studies were included in the qualitative syntheses and 39 in the quantitative ones. In permanent teeth, resin composite (RC) (RR = 2.00; 95%CI = 1.10, 3.64) and amalgam (AAG) (RR = 1.79; 95%CI = 1.04, 3.09) showed a higher risk of SC than Glass Ionomer Cement (GIC). In the deciduous teeth, however, a higher risk of SC was observed with RC than with AAG (RR = 2.46; 95%CI = 1.42, 4.27) and in GIC when compared to Resin-Modified Glass Ionomer Cement (RMGIC = 1.79; 95%CI = 1.04, 3.09). Most randomized clinical trials studies showed low or moderate risk of bias.
Conclusion: There is a difference between bioactive restorative materials for SC control, with GIC being more effective in the permanent teeth and the RMGIC in the deciduous teeth. Bioactive restorative materials can be adjuvants in the control of SC in patients at high risk for caries.
Keywords: Amalgam; Bioactive materials; Dental caries; Resin composite; Secondary caries.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures

Similar articles
-
Atraumatic restorative treatment versus conventional restorative treatment for managing dental caries.Cochrane Database Syst Rev. 2017 Dec 28;12(12):CD008072. doi: 10.1002/14651858.CD008072.pub2. Cochrane Database Syst Rev. 2017. PMID: 29284075 Free PMC article.
-
Dental fillings for the treatment of caries in the primary dentition.Cochrane Database Syst Rev. 2009 Apr 15;(2):CD004483. doi: 10.1002/14651858.CD004483.pub2. Cochrane Database Syst Rev. 2009. Update in: Cochrane Database Syst Rev. 2016 Oct 17;10:CD004483. doi: 10.1002/14651858.CD004483.pub3. PMID: 19370602 Updated.
-
Direct composite resin fillings versus amalgam fillings for permanent posterior teeth.Cochrane Database Syst Rev. 2021 Aug 13;8(8):CD005620. doi: 10.1002/14651858.CD005620.pub3. Cochrane Database Syst Rev. 2021. PMID: 34387873 Free PMC article.
-
The preventive effect of glass ionomer cement restorations on secondary caries formation: A systematic review and meta-analysis.Dent Mater. 2023 Dec;39(12):e1-e17. doi: 10.1016/j.dental.2023.10.008. Epub 2023 Oct 12. Dent Mater. 2023. PMID: 37838608
-
The preventive effect of glass ionomer restorations on new caries formation: A systematic review and meta-analysis.J Dent. 2022 Oct;125:104272. doi: 10.1016/j.jdent.2022.104272. Epub 2022 Aug 28. J Dent. 2022. PMID: 36038075
Cited by
-
Resin composite aggregated S-PRG particles are not superior to non-S-PRG under microcosm biofilm.Sci Rep. 2025 Jan 16;15(1):2173. doi: 10.1038/s41598-024-78396-1. Sci Rep. 2025. PMID: 39820496 Free PMC article.
-
Clinical performance and cost-effectiveness of low-shrinkage giomer resin composite versus resin-modified glass ionomer in cervical carious lesions: a 12-month randomized controlled trial.BMC Oral Health. 2025 Aug 6;25(1):1295. doi: 10.1186/s12903-025-06594-y. BMC Oral Health. 2025. PMID: 40770630 Free PMC article. Clinical Trial.
-
Clinical Effectiveness of Ion-Releasing Restorations versus Composite Restorations in Dental Restorations: Systematic Review and Meta-Analysis.Dent J (Basel). 2024 May 24;12(6):158. doi: 10.3390/dj12060158. Dent J (Basel). 2024. PMID: 38920859 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
