

Outcomes of patent foramen ovale greater than 3 mm at birth in extremely low birthweight infants
- PMID: 37322472
- PMCID: PMC10268431
- DOI: 10.1186/s12887-023-04119-6
Outcomes of patent foramen ovale greater than 3 mm at birth in extremely low birthweight infants
Abstract
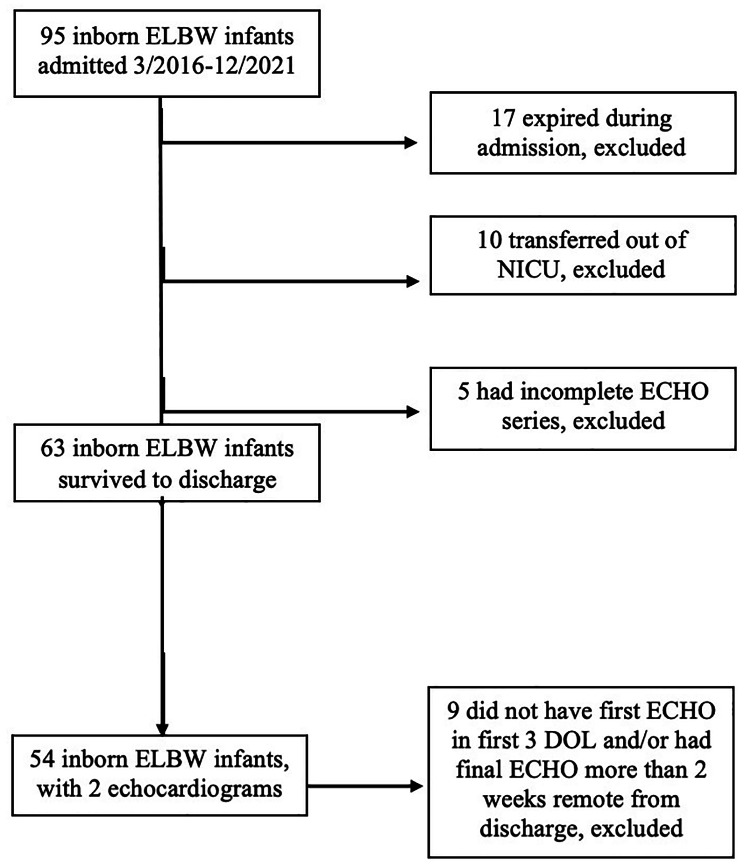
Background: Foramen ovale (FO) is an obligate fetal shunt that typically resolves after birth, although patency throughout life is not uncommon. The natural history of patent FO (PFO) is known in term infants, but less is known about its course in extremely preterm infants. We describe the echocardiographic changes in FO size from birth to discharge in extremely low birth weight (ELBW) infants in this retrospective study.
Methods: Cohort was divided based on size of FO at birth. Size of FO at discharge was measured and evaluated relative to postnatal weight gain. Demographics and clinical outcomes were compared between the two groups.
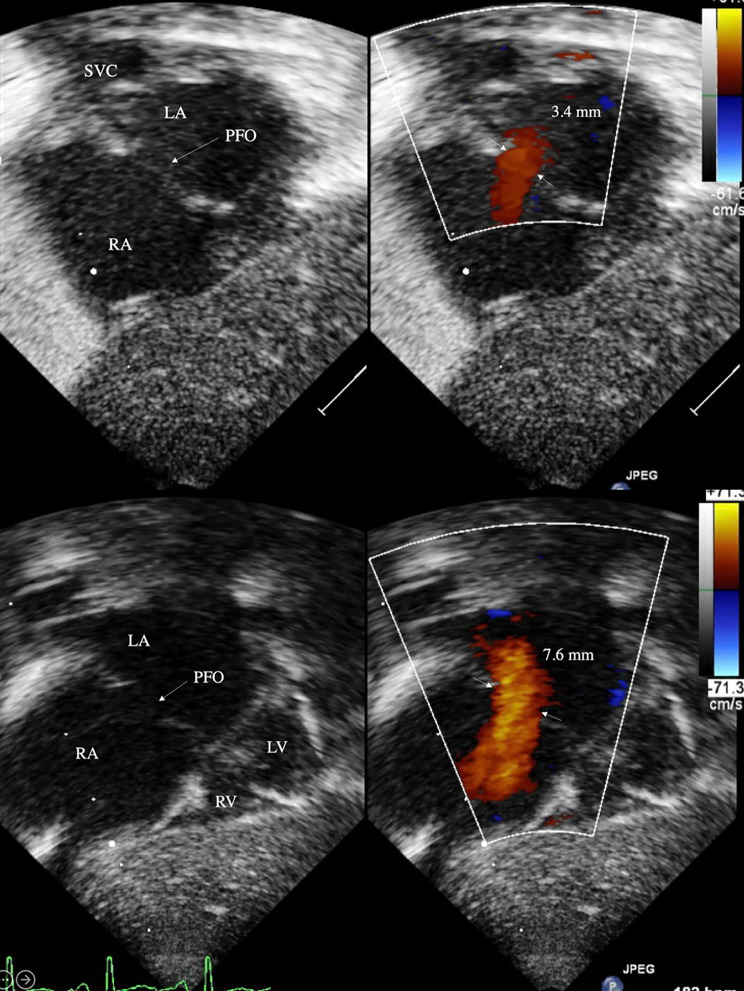
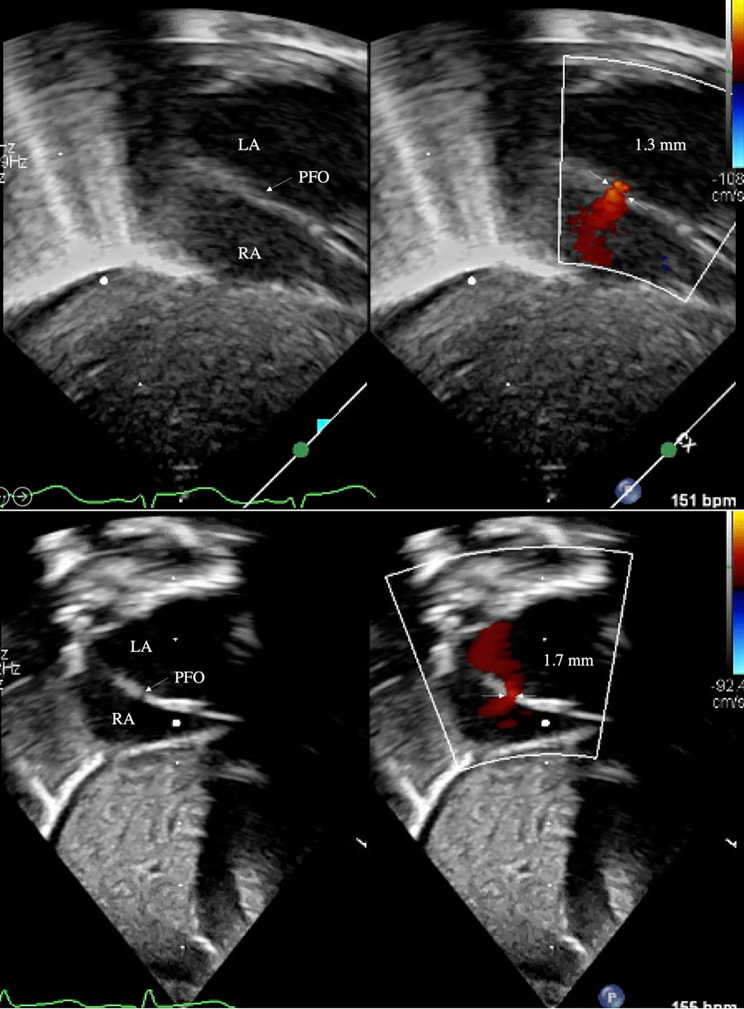
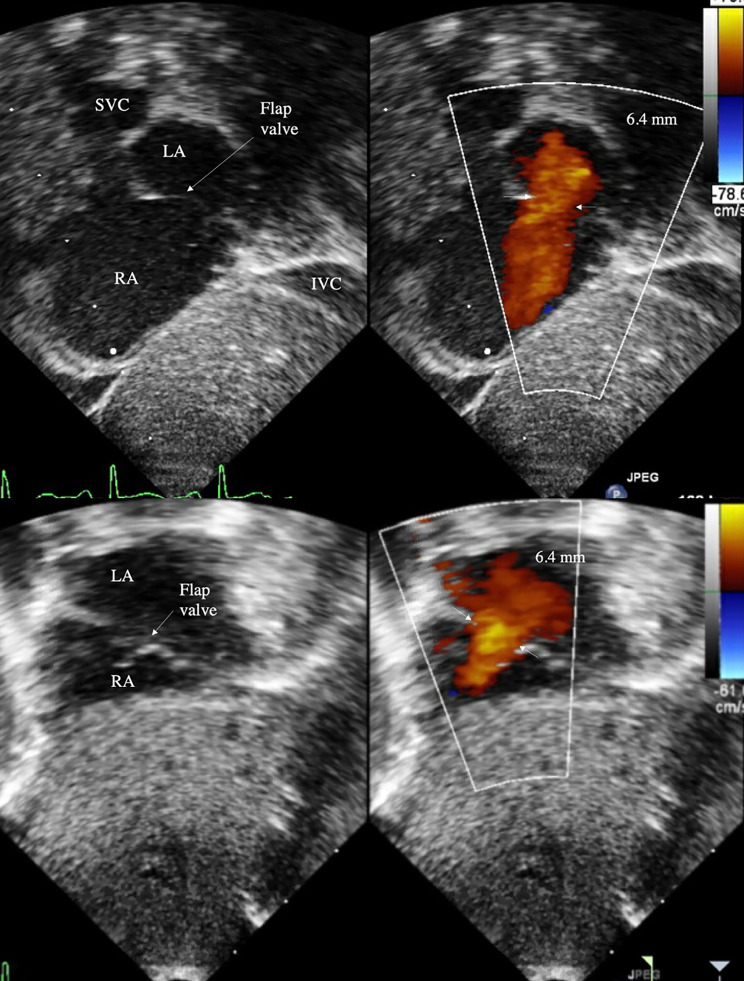
Results: Of the 54 ELBW infants, 50 were born with FO less than 3 mm in diameter (small), and 4 were born with FO greater than 3 mm (large). Of small defects, the majority (44/50, 88%) did not increase in size with weight gain, and minority (6/50, 12%) increased in size, and three of these 6 patients, FO grew to be slightly larger than 3 mm. In contrast, all large defects (4 of 4, 100%) nearly doubled in size with postnatal growth. These 4 ELBW infants with enlargement of FO had a flap valve evident on echocardiogram obtained prior to discharge, and subsequently closed on outpatient follow-up echocardiograms, although time to resolution was variable (6 months - 3 years). One infant had presumptive resolution because of the presence of flap valve.
Conclusion: No maternal or neonatal demographic characteristics were predictive of FO enlargement, although, demonstrable flap valve on discharge echocardiogram correlated with resolution of FO on outpatient follow-up echocardiogram. Therefore, based on our data, we recommend that ELBW infants born with large FO should have echocardiographic re-evaluation of the atrial septal opening prior to discharge, to specify the presence of a flap valve or lack thereof, which is an important detail that can help a neonatologist determine the need for outpatient cardiac follow-up.
Keywords: Extremely low birthweight; Flap valve; Neonatal echocardiography; Patent foramen ovale.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Pulmonary hemorrhage in extremely low birth weight infants: Significance of the size of left to right shunting through a valve incompetent patent foramen ovale.J Perinatol. 2022 Sep;42(9):1233-1237. doi: 10.1038/s41372-022-01464-9. Epub 2022 Jul 18. J Perinatol. 2022. PMID: 35851183
-
Benign outcome of pulmonary hypertension in neonates with a restrictive patent foramen ovale versus result for neonates with an unrestrictive patent foramen ovale.Pediatr Cardiol. 2011 Oct;32(7):972-6. doi: 10.1007/s00246-011-0032-7. Epub 2011 Jun 28. Pediatr Cardiol. 2011. PMID: 21710183
-
Weight gain in the first week of life and its association with morbidity and mortality in extremely low birthweight (ELBW) infants.Early Hum Dev. 2021 Sep;160:105421. doi: 10.1016/j.earlhumdev.2021.105421. Epub 2021 Jul 4. Early Hum Dev. 2021. PMID: 34256312
-
[Physiological and paraphysiological echocardiographic findings in neonatal and pediatric age].G Ital Cardiol (Rome). 2019 Nov;20(11):627-631. doi: 10.1714/3254.32223. G Ital Cardiol (Rome). 2019. PMID: 31697269 Review. Italian.
-
A Survey of Pediatric Cardiologists Regarding Non-emergent Echocardiographic Findings in Asymptomatic Newborns.Pediatr Cardiol. 2022 Apr;43(4):837-843. doi: 10.1007/s00246-021-02795-8. Epub 2022 Jan 9. Pediatr Cardiol. 2022. PMID: 34999921 Review.
Cited by
-
Descriptive analysis of colour Doppler echocardiography results in neonates with congenital heart disease in eastern China: a retrospective cohort study.Front Pediatr. 2025 Jul 31;13:1638808. doi: 10.3389/fped.2025.1638808. eCollection 2025. Front Pediatr. 2025. PMID: 40822684 Free PMC article.
References
-
- Bass JL et al. Embryology, neonatal circulation and anatomy of PFO. In: Amin Z editors. Patent Foramen Ovale, 1st edition. London: Springer; 2015. p. 7–14.
-
- Suradi H, Amin Z et al. Anatomical variations of patent foramen ovale. In: Amin Z editors. Patent Foramen Ovale, 1st edition. London: Springer; 2015. p. 15–24.
MeSH terms
LinkOut - more resources
Full Text Sources
