

Time to treatment and mortality for clinical sepsis subtypes
- PMID: 37322546
- PMCID: PMC10268363
- DOI: 10.1186/s13054-023-04507-5
Time to treatment and mortality for clinical sepsis subtypes
Abstract
Background: Sepsis is common, deadly, and heterogenous. Prior analyses of patients with sepsis and septic shock in New York State showed a risk-adjusted association between more rapid antibiotic administration and bundled care completion, but not an intravenous fluid bolus, with reduced in-hospital mortality. However, it is unknown if clinically identifiable sepsis subtypes modify these associations.
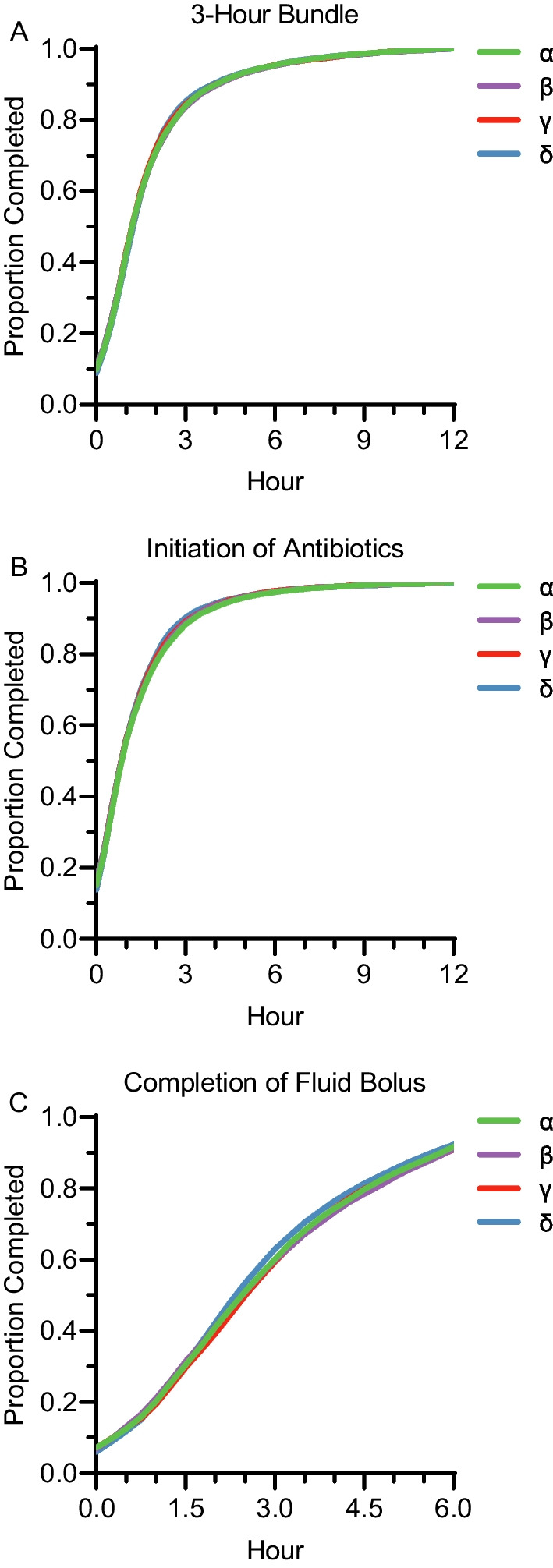
Methods: Secondary analysis of patients with sepsis and septic shock enrolled in the New York State Department of Health cohort from January 1, 2015 to December 31, 2016. Patients were classified as clinical sepsis subtypes (α, β, γ, δ-types) using the Sepsis ENdotyping in Emergency CAre (SENECA) approach. Exposure variables included time to 3-h sepsis bundle completion, antibiotic administration, and intravenous fluid bolus completion. Then logistic regression models evaluated the interaction between exposures, clinical sepsis subtypes, and in-hospital mortality.
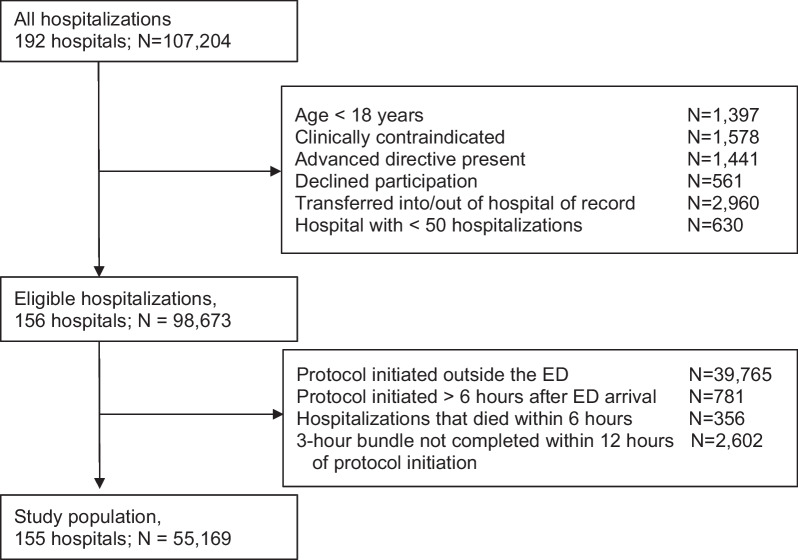
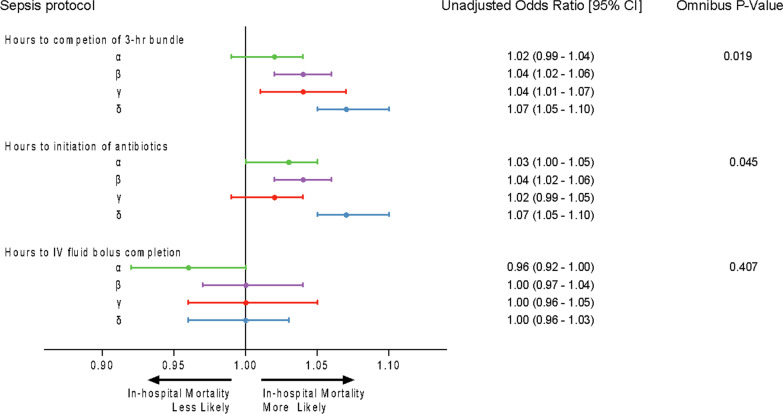
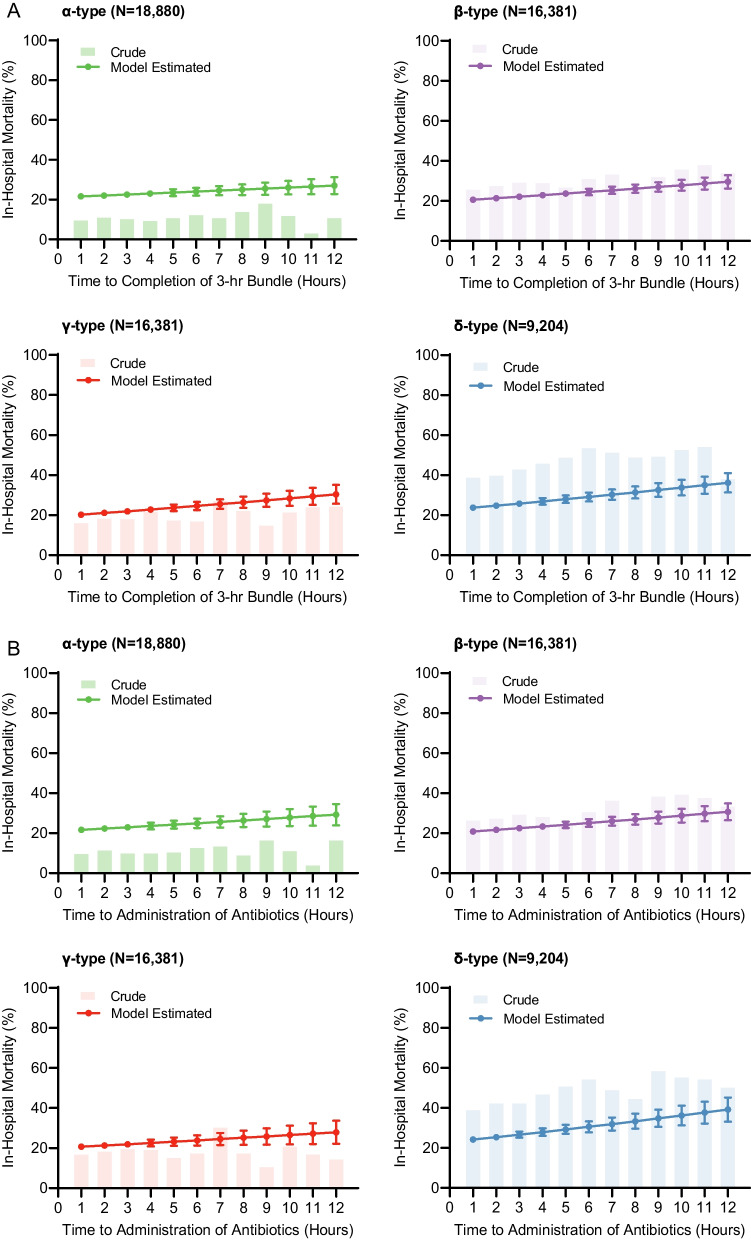
Results: 55,169 hospitalizations from 155 hospitals were included (34% α, 30% β, 19% γ, 17% δ). The α-subtype had the lowest (N = 1,905, 10%) and δ-subtype had the highest (N = 3,776, 41%) in-hospital mortality. Each hour to completion of the 3-h bundle (aOR, 1.04 [95%CI, 1.02-1.05]) and antibiotic initiation (aOR, 1.03 [95%CI, 1.02-1.04]) was associated with increased risk-adjusted in-hospital mortality. The association differed across subtypes (p-interactions < 0.05). For example, the outcome association for the time to completion of the 3-h bundle was greater in the δ-subtype (aOR, 1.07 [95%CI, 1.05-1.10]) compared to α-subtype (aOR, 1.02 [95%CI, 0.99-1.04]). Time to intravenous fluid bolus completion was not associated with risk-adjusted in-hospital mortality (aOR, 0.99 [95%CI, 0.97-1.01]) and did not differ among subtypes (p-interaction = 0.41).
Conclusion: Timely completion of a 3-h sepsis bundle and antibiotic initiation was associated with reduced risk-adjusted in-hospital mortality, an association modified by clinically identifiable sepsis subtype.
Keywords: Antibiotics; Precision medicine; Sepsis; Subtypes.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
