

Development of a dual energy CT based model to assess response to treatment in patients with high grade serous ovarian cancer: a pilot cohort study
- PMID: 37322564
- PMCID: PMC10268407
- DOI: 10.1186/s40644-023-00579-2
Development of a dual energy CT based model to assess response to treatment in patients with high grade serous ovarian cancer: a pilot cohort study
Abstract
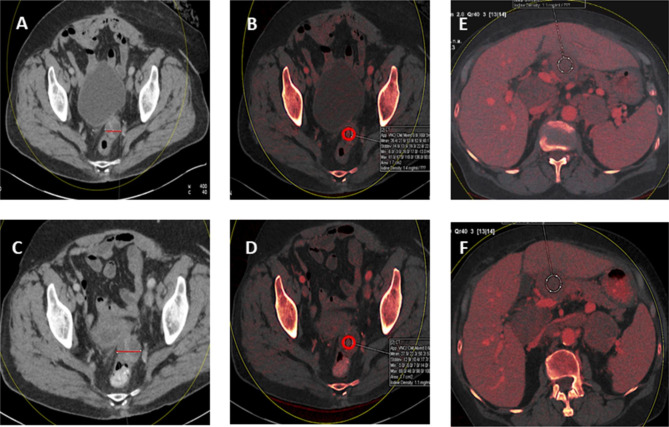
Background: In patients with cancer, the current gold standard for assessing response to treatment involves measuring cancer lesions on computed tomography (CT) imaging. The percentage change in size of specific lesions determines whether patients have had a complete/partial response or progressive disease, according to RECIST criteria. Dual Energy CT (DECT) permits additional measurements of iodine concentration, a surrogate marker of vascularity. Here we explore the role of changes in iodine concentration within cancer tissue on CT scans to assess its suitability for determining treatment response in patients with high grade serous ovarian cancer (HGSOC).
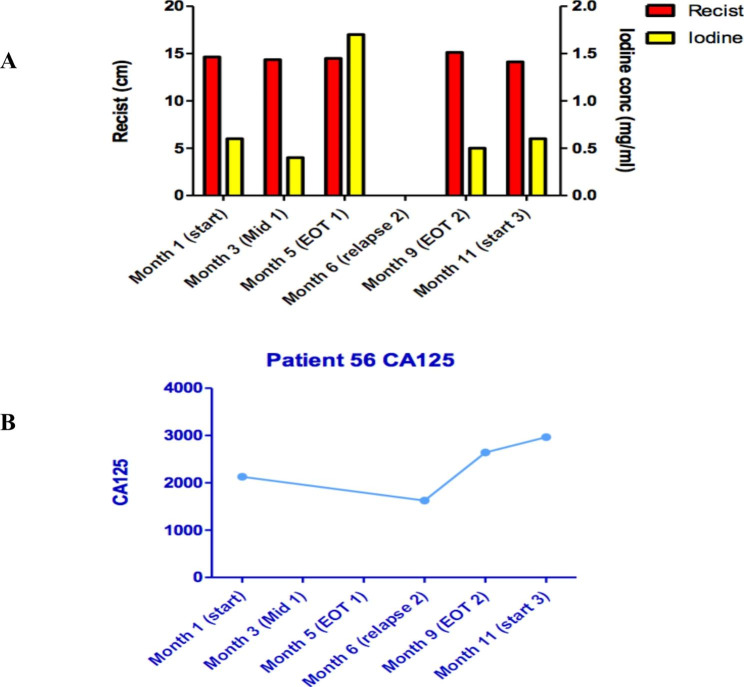
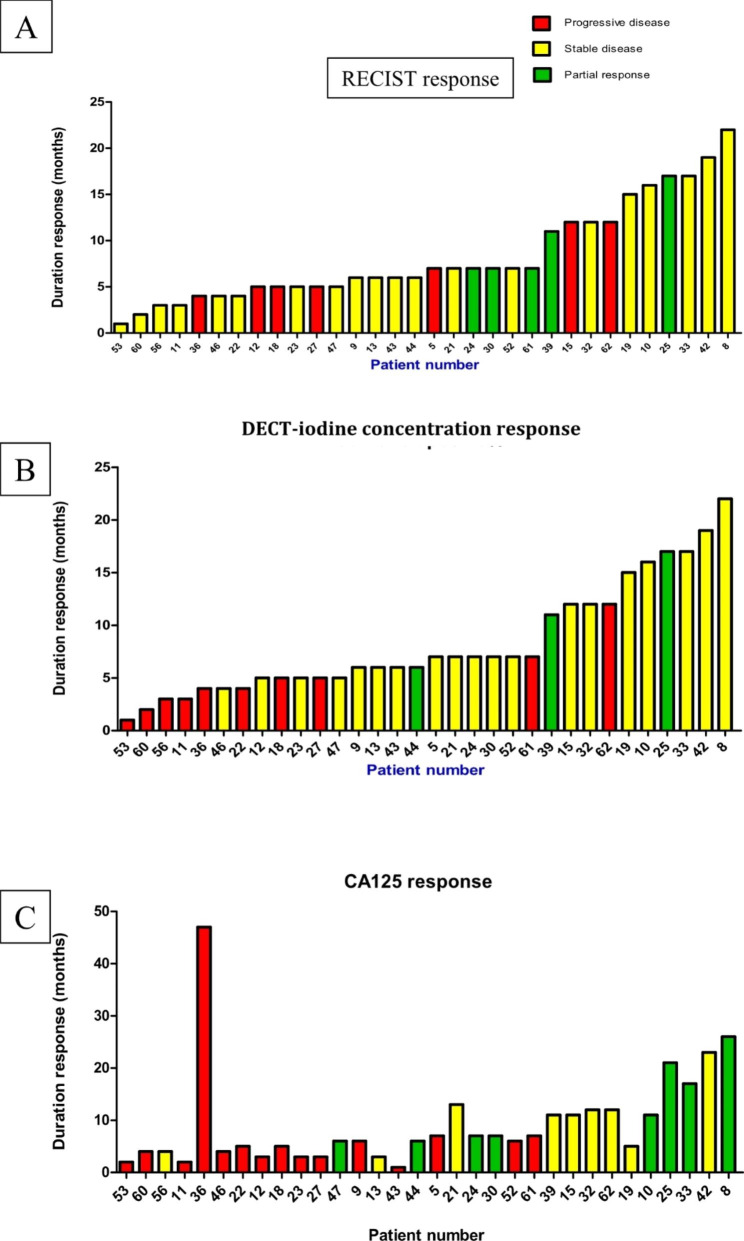
Methods: Suitable RECIST measurable lesions were identified from the CT images of HGSOC patients, taken at 2 different time points (pre and post treatment). Changes in size and iodine concentration were measured for each lesion. PR/SD were classified as responders, PD was classified as non-responder. Radiological responses were correlated with clinical and CA125 outcomes.
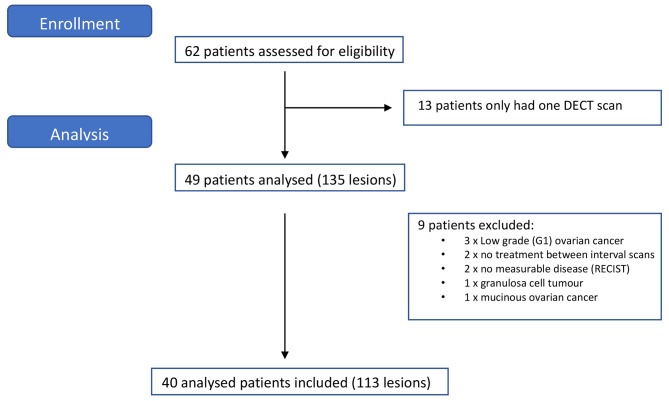
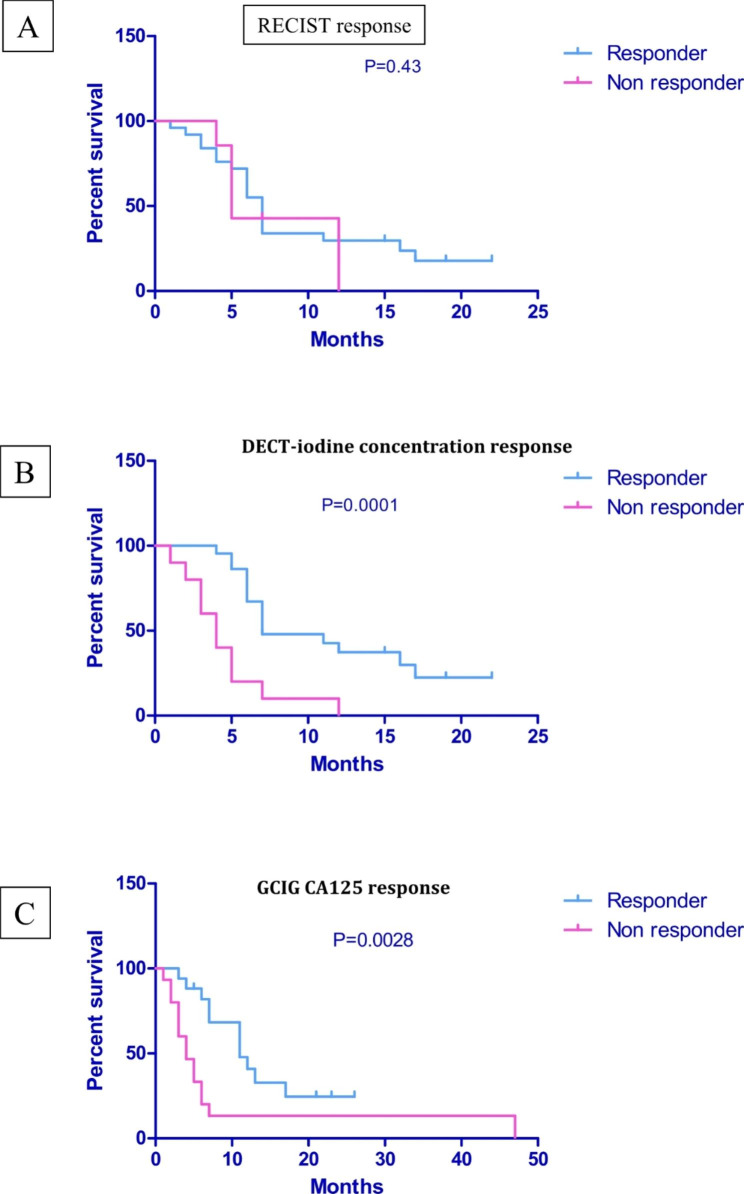
Results: 62 patients had appropriate imaging for assessment. 22 were excluded as they only had one DECT scan. 32/40 patients assessed (113 lesions) had received treatment for relapsed HGSOC. RECIST and GCIG (Gynaecologic Cancer Inter Group) CA125 criteria / clinical assessment of response for patients was correlated with changes in iodine concentration, before and after treatment. The prediction of median progression free survival was significantly better associated with changes in iodine concentration (p = 0.0001) and GCIG Ca125 / clinical assessment (p = 0.0028) in comparison to RECIST criteria (p = 0.43).
Conclusion: Changes in iodine concentration from dual energy CT imaging may be more suitable than RECIST in assessing response to treatment in patients with HGSOC.
Trial registration: CICATRIx IRAS number 198179, 14 Dec 2015, https://www.myresearchproject.org.uk/ .
Keywords: Dual energy CT; GCIG CA125; High grade serous ovarian cancer (HGSOC); Iodine concentration; Progression free survival (PFS); RECIST.
© 2023. The Author(s).
Conflict of interest statement
Disclosure the authors have no conflicts of interest with respect to this work.
Figures
References
-
- Ovarian cancer [Internet]. Ovarian cancer. [cited 2021 May 20]. Available from: https://www.cancerresearchuk.org/about-cancer/ovarian-cancer.
-
- Fischerova D, Burgetova A. Imaging techniques for the evaluation of ovarian cancer. Best Pract Res Clin Obstet Gynaecol. 2014 Jul;28(5). - PubMed
-
- Eisenhauer ETPBJ et al. New response evaluation criteria in tumors: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;(45):228–47. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
