

Heterogeneous Comorbidity in Individuals With Different Phenotypes of Obesity
- PMID: 37323325
- PMCID: PMC10262764
- DOI: 10.7759/cureus.38995
Heterogeneous Comorbidity in Individuals With Different Phenotypes of Obesity
Abstract
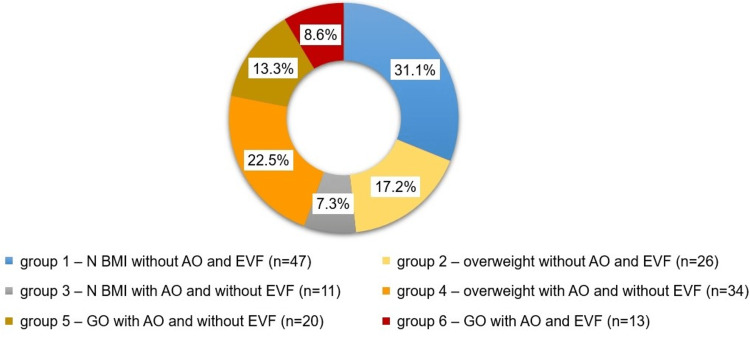
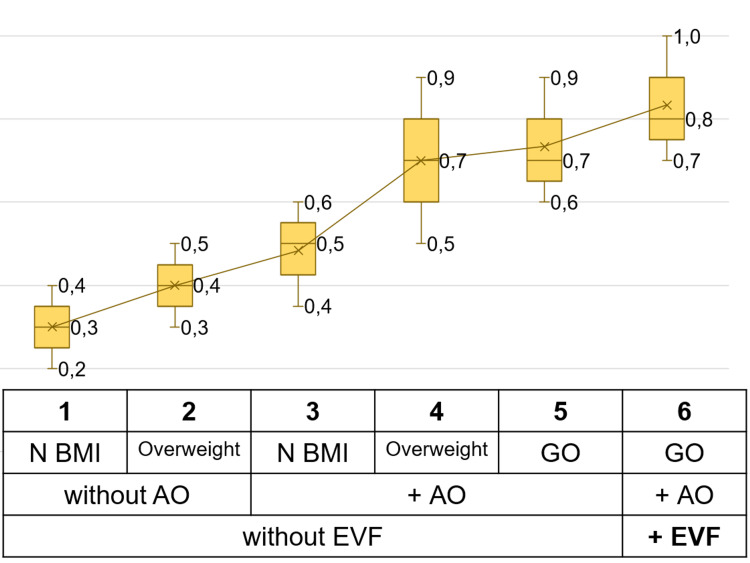
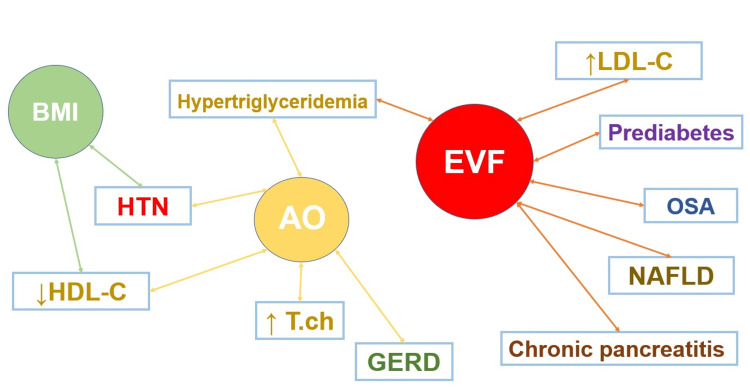
Introduction The prevalence of obesity is steadily increasing worldwide. Obesity is one of the most potent risk factors for various diseases and is simultaneously a heterogeneous condition. Different types of obesity could be identified according to body mass index (BMI), waist circumference, and visceral fat level; these conditions may present individually or in combination and pose a risk of developing certain comorbidities. However, the current obesity classification systems do not allow for accurate diagnosis and prediction of the comorbidity risk of patients, which is crucial for their clinical management. This points to the importance of studying obesity phenotyping in the context of body composition. Our study aimed to determine the contribution of obesity phenotypes in forming various comorbidities. Materials and methods This case-control study was conducted at the Clinical and Diagnostic Center of the Aviastroitelny District, Kazan. Patients were selected based on BMI per inclusion and exclusion criteria. A total of 151 patients with a median age of 43 [34.5-50] years were included in the study. The participants were distributed into six groups according to BMI and a combination of abdominal obesity (AO) and excess visceral fat. Results The participants were distributed in the following phenogroups: The first group - normal BMI without AO and excess visceral fat (n=47; 31.1%); the second group - overweight without AO and excess visceral fat (n=26; 17.2%); the third group - normal BMI with AO and without excess visceral fat (n=11; 7.3%); fourth group - overweight with AO and without excess visceral fat (n=34; 22.5%); fifth group - general obesity with AO and without excess visceral fat (n=20; 13.2%); sixth group - general obesity with AO and excess visceral fat (n=13; 8.6%). The five most frequently observed conditions in the general cohort were dyslipidemia (71.5%; n=108), disorders of the gastrointestinal tract (53.0%; n=80), cardiovascular disease (46.4%; n=70), musculoskeletal diseases (40.4%; n=61) and impaired carbohydrate metabolism (25.2%; n=38). The median number of pathological combinations in the general cohort was 5 [IQR: 3-7]. As the group number increased, the median number of comorbidities also increased. While BMI was significantly associated only with arterial hypertension, the level of visceral fat was associated with most comorbidities (obstructive sleep apnea syndrome, non-alcoholic fatty liver disease, chronic pancreatitis, hypertriglyceridemia, and prediabetes), followed by abdominal obesity (gastroesophageal reflux disease, hypertriglyceridemia, arterial hypertension, hypercholesterolemia). Conclusions In working-age people, group 1 and 4 phenotypes were more frequent than others. Abdominal obesity and visceral fat were associated with the most comorbid conditions. However, the individual types of these comorbidities were not the same.
Keywords: abdominal obesity; comorbidity; obesity; obesity phenotypes; visceral obesity.
Copyright © 2023, Nurieva et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Obesity and overweight. [ Jan; 2023 ]. 2021. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
-
- The profile of risk factors for chronic non-communicable diseases among distinct phenotypes of obesity [Russian] Nurieva AR, Sineglazova AV, Kim TY, Parve S. Bull Contemp Clin Med. 2021;14:41–46.
LinkOut - more resources
Full Text Sources
Research Materials