

Bacteremia During the First Year After Solid Organ Transplantation: An Epidemiological Update
- PMID: 37323422
- PMCID: PMC10267299
- DOI: 10.1093/ofid/ofad247
Bacteremia During the First Year After Solid Organ Transplantation: An Epidemiological Update
Abstract
Background: There are limited contemporary data on the epidemiology and outcomes of bacteremia in solid organ transplant recipients (SOTr).
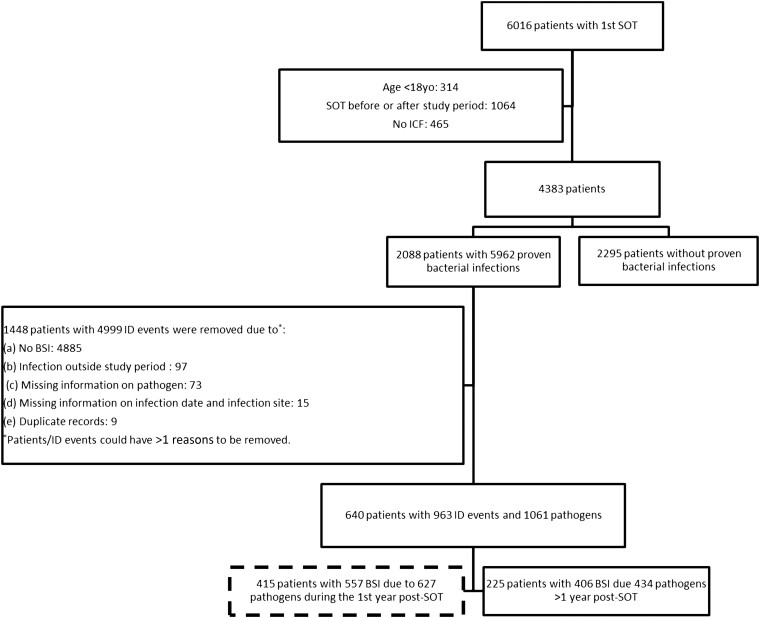
Methods: Using the Swiss Transplant Cohort Study registry from 2008 to 2019, we performed a retrospective nested multicenter cohort study to describe the epidemiology of bacteremia in SOTr during the first year post-transplant.
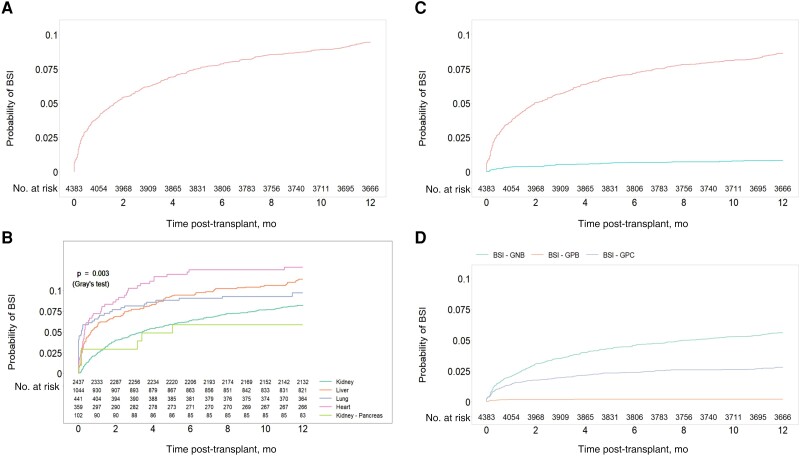
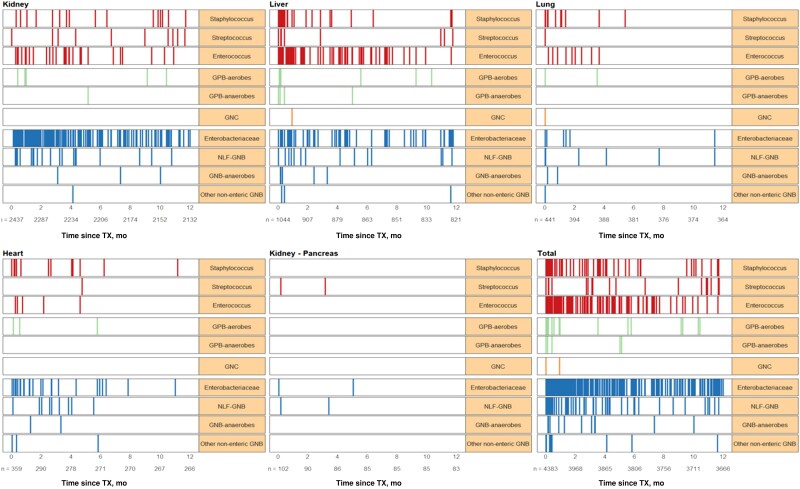
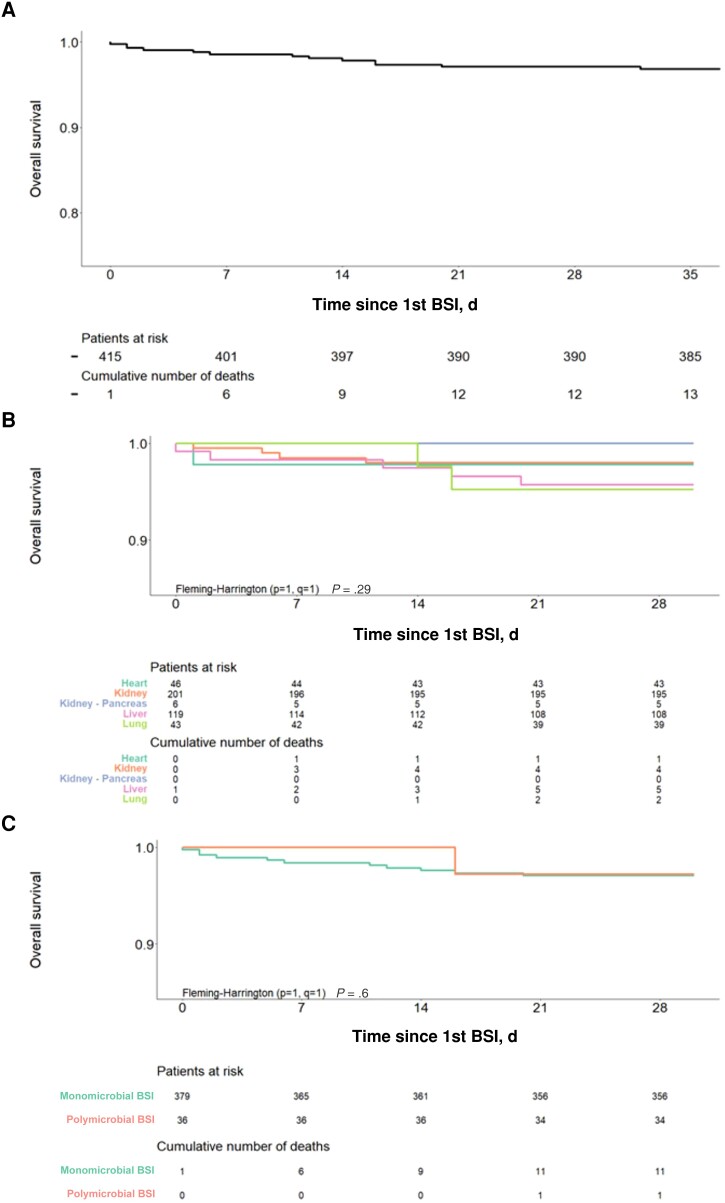
Results: Of 4383 patients, 415 (9.5%) with 557 cases of bacteremia due to 627 pathogens were identified. One-year incidence was 9.5%, 12.8%, 11.4%, 9.8%, 8.3%, and 5.9% for all, heart, liver, lung, kidney, and kidney-pancreas SOTr, respectively (P = .003). Incidence decreased during the study period (hazard ratio, 0.66; P < .001). One-year incidence due to gram-negative bacilli (GNB), gram-positive cocci (GPC), and gram-positive bacilli (GPB) was 5.62%, 2.81%, and 0.23%, respectively. Seven (of 28, 25%) Staphylococcus aureus isolates were methicillin-resistant, 2/67 (3%) enterococci were vancomycin-resistant, and 32/250 (12.8%) GNB produced extended-spectrum beta-lactamases. Risk factors for bacteremia within 1 year post-transplant included age, diabetes, cardiopulmonary diseases, surgical/medical post-transplant complications, rejection, and fungal infections. Predictors for bacteremia during the first 30 days post-transplant included surgical post-transplant complications, rejection, deceased donor, and liver and lung transplantation. Transplantation in 2014-2019, CMV donor-negative/recipient-negative serology, and cotrimoxazole Pneumocystis prophylaxis were protective against bacteremia. Thirty-day mortality in SOTr with bacteremia was 3% and did not differ by SOT type.
Conclusions: Almost 1/10 SOTr may develop bacteremia during the first year post-transplant associated with low mortality. Lower bacteremia rates have been observed since 2014 and in patients receiving cotrimoxazole prophylaxis. Variabilities in incidence, timing, and pathogen of bacteremia across different SOT types may be used to tailor prophylactic and clinical approaches.
Keywords: bacteremia; bloodstream infection; clinical outcomes; epidemiology; risk factors; solid organ transplant; timing.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. All authors: no reported conflicts.
Figures

References
-
- Ye QF, Zhao J, Wan QQ, Qiao BB, Zhou JD. Frequency and clinical outcomes of ESKAPE bacteremia in solid organ transplantation and the risk factors for mortality. Transpl Infect Dis 2014; 16:767–74. - PubMed
-
- Shao MJ, Wan QQ, Xie WZ, Ye QF. Bloodstream infections among solid organ transplant recipients: epidemiology, microbiology, associated risk factors for morbility and mortality. Transplant Rev-Orlan 2014; 28:176–81. - PubMed
-
- Gavalda J, Aguado JM, Manuel O, Grossi P, Hirsch HH; ESCMID Study Group of Infection in Compromised Hosts . . A special issue on infections in solid organ transplant recipients. Clin Microbiol Infect 2014; 20(Suppl 7):1–3. - PubMed
-
- Bodro M, Sabe N, Tubau F, et al. . Risk factors and outcomes of bacteremia caused by drug-resistant ESKAPE pathogens in solid-organ transplant recipients. Transplantation 2013; 96:843–9. - PubMed
-
- Rodriguez C, Munoz P, Rodriguez-Creixems M, Yanez JF, Palomo JS, Bouza E. Bloodstream infections among heart transplant recipients. Transplantation 2006; 81:384–91. - PubMed
