

Analyzing the impact of minimally invasive surgical approaches on post-operative outcomes of pneumonectomy and sleeve lobectomy patients
- PMID: 37324102
- PMCID: PMC10267906
- DOI: 10.21037/jtd-22-654
Analyzing the impact of minimally invasive surgical approaches on post-operative outcomes of pneumonectomy and sleeve lobectomy patients
Abstract
Background: Some patients with non-small cell lung cancer (NSCLC) have superior short- and long-term outcomes with sleeve lobectomy rather than pneumonectomy. Originally sleeve lobectomy was reserved for patients with limited pulmonary function, however, the reported superior results allowed sleeve lobectomy to be performed in expanded patient populations. In a further attempt to improve post-operative outcomes surgeons have adopted minimally invasive techniques Minimally invasive approaches have potential benefits to patients such as decreased morbidity and mortality while maintaining the same caliber of oncologic outcomes.
Methods: We identified patients at our institution who underwent sleeve lobectomy or pneumonectomy to treat NSCLC from 2007 to 2017. We analyzed these groups in respect to 30- and 90-day mortality, complications, local recurrence, and median survival. We included multivariate analysis to determine the impact of a minimally invasive approach, sex, extent of resection, and histology. Differences in mortality were analyzed using the Kaplan-Meier method using the log-rank test to compare the groups. A two-tailed Z test for difference in proportions was done to analyze complications, local recurrence, 30-day and 90-day mortality.
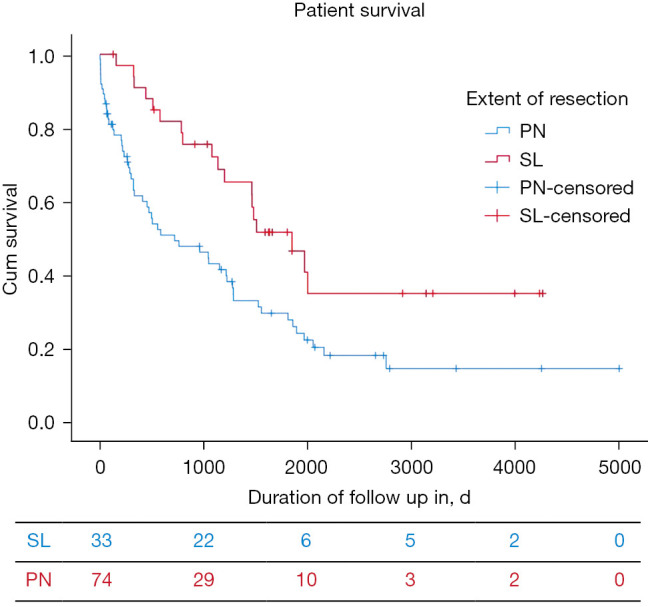
Results: A total of 108 patients underwent sleeve lobectomy (n=34) or pneumonectomy (n=74) for treatment of NSCLC with 18 undergoing open pneumonectomy, 56 undergoing video-assisted thoracoscopic surgery (VATS) pneumonectomy, 29 undergoing open sleeve lobectomy, and 5 undergoing VATS sleeve lobectomy. There was no significant difference in 30-day mortality (P=0.064) but there was a difference in 90-day (P=0.007). There was no difference in complication rates (P=0.234) or local recurrence rates (P=0.779). The pneumonectomy patients had a median survival of 23.6 months (95% CI: 3.8-43.4 months). The sleeve lobectomy group had a median survival of 60.7 months (95% CI: 43.3-78.2 months) (P=0.008). On multivariate analysis extent of resection (P<0.001) and tumor stage (P=0.036) were associated with survival. There was no significant difference between the VATS approach and the open surgical approach (P=0.053).
Conclusions: When considering patients undergoing surgery for NSCLC sleeve lobectomy resulted in lower 90-day mortality and better 3-year survival compared to patients undergoing PN. Having a sleeve lobectomy rather than a pneumonectomy and having earlier-stage disease lead to significantly improved survival on multivariate analysis. Having a VATS operation leads to a non-inferior post-operative outcome compared to open surgery.
Keywords: Lung cancer; pneumonectomy (PN); sleeve lobectomy (SL); video-assisted thoracoscopic surgery (VATS).
2023 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-654/coif). The authors have no conflicts of interest to declare.
Figures
Comment in
-
Patient selection for minimally-invasive resection of complex, central lung tumors: taking account of the surgeon's eyeball test.J Thorac Dis. 2023 Jul 31;15(7):3522-3524. doi: 10.21037/jtd-23-715. Epub 2023 Jul 4. J Thorac Dis. 2023. PMID: 37559641 Free PMC article. No abstract available.
References
-
- Collins LG, Haines C, Perkel R, et al. Lung cancer: diagnosis and management. Am Fam Physician 2007;75:56-63. - PubMed
LinkOut - more resources
Full Text Sources