

Extended Level IV Neck Dissection for Limited Prophylactic Clearance of Level V in Node-Positive Papillary Thyroid Carcinoma: a Homogenous Study Population
- PMID: 37324295
- PMCID: PMC10267089
- DOI: 10.1007/s13193-020-01167-7
Extended Level IV Neck Dissection for Limited Prophylactic Clearance of Level V in Node-Positive Papillary Thyroid Carcinoma: a Homogenous Study Population
Abstract
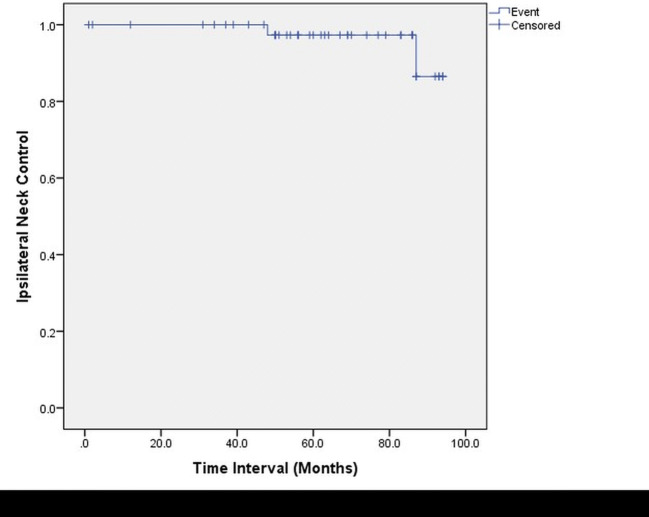
There is near consensus that prophylactic lateral neck dissection has no role in the management of differentiated thyroid cancer, but the extent of lateral neck dissection in differentiated thyroid cancer remains controversial, especially whether level V should be addressed or not. There is lot of heterogeneity in reporting of the management of level V in papillary thyroid cancer. We at our Institute address the lateral neck positive papillary thyroid cancer with selective neck dissection involving levels II-IV, performing extended level IV dissection with inclusion of the triangular area delineated by the sternocleidomastoid muscle, the clavicle, and the perpendicular line drawn to the clavicle from the point where the horizontal line at the level of cricoid cuts the posterior border of sternocleidomastoid muscle. Retrospective analysis of the departmental data set related to thyroidectomy with lateral neck dissection from 2013 to mid-2019 for papillary thyroid cancer, was carried out. Patients with recurrent papillary thyroid cancer were excluded as were patients with involvement of level V. Data related to the demography of patients, histological diagnosis, and postoperative complications were compiled and summarized. Note was made of the incidence of ipsilateral neck recurrence and the neck level involved with recurrence noted. Data was analyzed for fifty-two patients of non-recurrent papillary thyroid cancer who had undergone total thyroidectomy and lateral neck dissection involving levels II-IV, with extended dissection at level IV. It should be noted that none of the patients had clinical involvement of level V. Only two patients had lateral neck recurrence, both the recurrences were in level III, one on the ipsilateral side and the other on the contralateral side. Recurrence in the central compartment was noted in two patients, with one of these patients also having ipsilateral level III recurrence. One of the patients had distal metastasis to the lungs. Transient paresis of the unilateral vocal cords was noted in seven patients which got resolved within 2 months in all of them. Transient hypocalcemia was noted in four patients. Although our series has a small sample size with limited follow-up, it is one of the few studies in which prophylactic level V dissection has been studied in a homogenous study population of non-recurrent papillary thyroid cancer. Our study has shown that prophylactic dissection of level V may have a limited role, but further large multi-institutional studies need to be carried out to come up with a definite answer.
Keywords: Limited prophylactic clearance; Prophylactic lateral neck dissection; Thyroid cancer.
© Indian Association of Surgical Oncology 2020.
Conflict of interest statement
Conflict of InterestThe authors declare that they have no conflict of interest.
Figures

Similar articles
-
Robot-assisted Sistrunk's operation, total thyroidectomy, and neck dissection via a transaxillary and retroauricular (TARA) approach in papillary carcinoma arising in thyroglossal duct cyst and thyroid gland.Ann Surg Oncol. 2012 Dec;19(13):4259-61. doi: 10.1245/s10434-012-2674-y. Epub 2012 Oct 16. Ann Surg Oncol. 2012. PMID: 23070784
-
Robotic total thyroidectomy with modified radical neck dissection via unilateral retroauricular approach.Ann Surg Oncol. 2014 Nov;21(12):3872-5. doi: 10.1245/s10434-014-3896-y. Epub 2014 Sep 17. Ann Surg Oncol. 2014. PMID: 25227305
-
Role and Extent of Neck Dissection for Neck Lymph Node Metastases in Differentiated Thyroid Cancers.Sisli Etfal Hastan Tip Bul. 2021 Dec 29;55(4):438-449. doi: 10.14744/SEMB.2021.76836. eCollection 2021. Sisli Etfal Hastan Tip Bul. 2021. PMID: 35317376 Free PMC article. Review.
-
Total thyroidectomy with therapeutic level II-IV neck dissection for papillary thyroid carcinoma: level VI recurrence patterns.Eur Arch Otorhinolaryngol. 2020 Dec;277(12):3449-3455. doi: 10.1007/s00405-020-06079-4. Epub 2020 Jun 2. Eur Arch Otorhinolaryngol. 2020. PMID: 32488373
-
Clinical significance of prophylactic central compartment neck dissection in the treatment of clinically node-negative papillary thyroid cancer patients.World J Surg Oncol. 2016 Sep 19;14(1):247. doi: 10.1186/s12957-016-1003-5. World J Surg Oncol. 2016. PMID: 27644091 Free PMC article. Review.
References
-
- Leenhardt L, Erdogan MF, Hegedus L, Mandel SJ, Paschke R, Rago T, Russ G. European Thyroid Association guidelines for cervical ultrasound scan and ultrasound-guided techniques in the postoperative management of patients with thyroid cancer. Eur Thyroid J. 2013;2:147–159. doi: 10.1159/000354537. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources