

Fluoroscopic Stent Placement as a Bridge to Surgery for Malignant Colorectal Obstruction: Short- and Long-Term Outcomes
- PMID: 37324992
- PMCID: PMC10265237
- DOI: 10.3348/jksr.2022.0097
Fluoroscopic Stent Placement as a Bridge to Surgery for Malignant Colorectal Obstruction: Short- and Long-Term Outcomes
Abstract
Purpose: To assess the outcomes of single-stage surgery following fluoroscopic stent placement for malignant colorectal obstruction.
Materials and methods: This retrospective study included 46 patients (28 male and 18 female; mean age, 67.2 years) who had undergone fluoroscopic stent placement followed by laparoscopic resection (n = 31) or open surgery (n = 15) for malignant colorectal obstruction. The surgical outcomes were analyzed and compared. After a mean follow-up of 38.9 months, the recurrence-free and overall survival were estimated, and prognostic factors were evaluated.
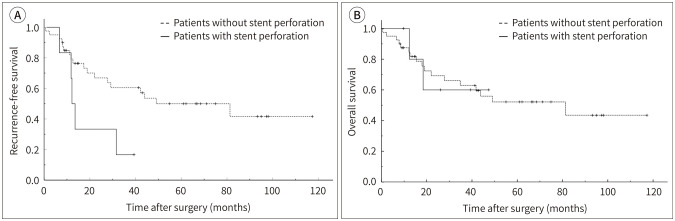
Results: The mean interval between stent placement and surgery was 10.2 days. Primary anastomosis was possible in all patients. The mean postoperative length of hospitalization was 11.0 days. Bowel perforation was detected in six patients (13.0%). During the follow-up, ten patients (21.7%) developed recurrence; these included five of the six patients with bowel perforation. Bowel perforation had a significant effect on recurrence-free survival (p = 0.010).
Conclusion: Single-stage surgery following fluoroscopic stent placement may be effective for treating malignant colorectal obstruction. Stent-related bowel perforation is a significant predictive factor for tumor recurrence.
목적: 악성대장협착에서 스텐트 설치 후 시행한 단단계 수술의 결과를 평가하고자 하였다.
대상과 방법: 2009년 1월부터 2018년 1월까지, 악성대장협착으로 투시장치 하 스텐트를 설치하여 장세척을 한 후 수술을 시행한 46명의 환자(남:여 = 28:18, 평균 67.2세)를 대상으로 하였다. 그중 31명은 복강경수술, 15명은 개복수술을 시행하였으며, 수술 결과를 후향적으로 분석하였다. 평균 38.9개월의 추적관찰 기간 동안, 무재발생존율과 전체생존율을 구하였고, 예후인자를 알아보았다.
결과: 스텐트 설치 후 평균 10.2일 후에 수술을 시행하였으며, 전례에서 성공적으로 스텐트를 포함한 종양 절제 후 문합이 가능하였다. 수술 후 평균 입원기간은 11일이었다. 6명의 환자(13%)에서 수술 중 혹은 수술 후 병리 소견에서 장천공이 관찰되었다. 추적 기간 동안 10명의 환자(21.7%)에서 종양이 재발하였으며, 장천공이 관찰되었던 6명의 환자 중 5명에서 재발이 발생하였다. 장천공은 무재발생존율에 유의미한 영향을 미쳤다(p = 0.010).
결론: 악성대장협착에서 스텐트 설치 후 시행한 단단계 수술은 효과적인 치료 방법으로 생각된다. 스텐트와 연관된 장천공이 재발의 위험인자였다.
Keywords: Colorectal Neoplasms; Intestinal Obstruction; Laparoscopy; Self Expandable Metallic Stents.
Copyrights © 2023 The Korean Society of Radiology.
Conflict of interest statement
Conflicts of Interest: The authors have no potential conflicts of interest to disclose.
Figures

References
-
- Deans GT, Krukowski ZH, Irwin ST. Malignant obstruction of the left colon. Br J Surg. 1994;81:1270–1276. - PubMed
-
- Leitman IM, Sullivan JD, Brams D, DeCosse JJ. Multivariate analysis of morbidity and mortality from the initial surgical management of obstructing carcinoma of the colon. Surg Gynecol Obstet. 1992;174:513–518. - PubMed
-
- Biondo S, Parés D, Frago R, Martí-Ragué J, Kreisler E, De Oca J, et al. Large bowel obstruction: predictive factors for postoperative mortality. Dis Colon Rectum. 2004;47:1889–1897. - PubMed
-
- Zorcolo L, Covotta L, Carlomagno N, Bartolo DC. Safety of primary anastomosis in emergency colo-rectal surgery. Colorectal Dis. 2003;5:262–269. - PubMed
-
- Mainar A, De Gregorio Ariza MA, Tejero E, Tobío R, Alfonso E, Pinto I, et al. Acute colorectal obstruction: treatment with self-expandable metallic stents before scheduled surgery--results of a multicenter study. Radiology. 1999;210:65–69. - PubMed
LinkOut - more resources
Full Text Sources
