

Clinical Characteristics and Oncological Outcomes of Surgically Treated Early-Onset Gastric Adenocarcinoma - a Retrospective Cohort Study
- PMID: 37325055
- PMCID: PMC10266247
- DOI: 10.7150/jca.82876
Clinical Characteristics and Oncological Outcomes of Surgically Treated Early-Onset Gastric Adenocarcinoma - a Retrospective Cohort Study
Abstract
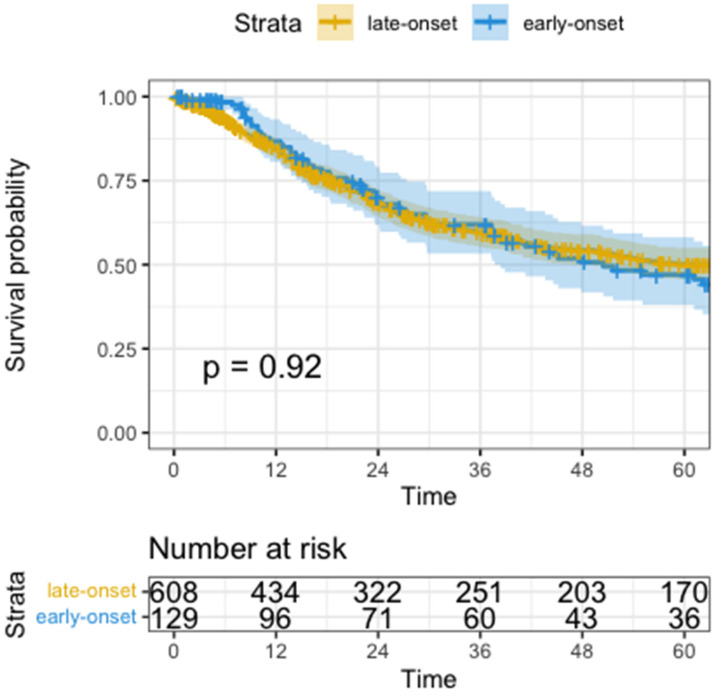
Introduction: The incidence of early-onset gastric adenocarcinoma (patients <50 years, EOGA) is rising. Tumors in younger patients are associated with prognostically unfavorable features. The impact of EOGA on patient survival, however, remains unclear. The aim of this study is to evaluate early-onset age as a prognostic factor compared to late-onset gastric adenocarcinoma (LOGA, >50years) in a surgical cohort and assess treatment options. Methods: We analyzed 738 patients (129 early-onset/609 late-onset) operated in curative intent from 2002 to 2021. Data was extracted from a prospectively managed database of an academic tertiary referral hospital. Differences in perioperative as well as oncological outcomes were calculated by chi-square test. Cox regression analysis was performed to assess disease-free survival (DFS) and overall survival (OS). Results: EOGA patients were more often treated with neoadjuvant therapy (62.8% vs. 43.7%, p<0.001) and extended surgical resections e.g. through additional resections (36.4% vs. 26.8%, p=0.027). EOGA was more often metastasized into regional lymph nodes (pN+ 67.4% vs. 55.3%, p=0.012) and to distant sites (pM+: 23.3% vs. 12.0%, p=0.001) and was more often poorly differentiated (G3/G4: 91.1% vs. 67.2%, p<0.001). There were no significant differences in overall complication rates (31.0% vs. 36.6%, p=0.227). Survival analysis showed shorter DFS (median DFS 25.6 months vs. not reached, p=0.006) but similar OS (median OS: 50.5 months vs. not reached, p=0.920) in EOGA compared to LOGA. Conclusions: This analysis confirmed that EOGA is associated with more aggressive tumor characteristics. Early-Onset was not a prognostic factor in the multivariate analysis. EOGA patients may be more capable to undergo intensive multimodal therapy including perioperative chemotherapy and extended surgery.
Keywords: adenocarcinoma; early-onset; gastric cancer; surgery; young.
© The author(s).
Conflict of interest statement
Competing Interests: G.M. H. reported to having received the following funding unrelated to this manuscript: Consulting or Advisory Role: Bristol-Myers Squibb; MSD Sharp & Dohme; Lilly; Novartis; Daiichi Sankyo. Honoraria: Servier; MSD Sharp & Dohme; Lilly; Targos; Bristol-Myers Squibb; IOMEDICO, MCI Conventions. Research Funding (not related to this manuscript): Nordic Pharma; Taiho Pharmaceutical; MSD Sharp & Dohme; Janssen; Astra Zeneca; Bristol-Myers Squibb; IKF Klinische Krebsforschung Frankfurt. Travel; Accommodations: Bristol-Myers Squibb; Lilly; Servier; MSD Sharp & Dohme. All other authors stated no conflict of interest.
Figures



Similar articles
-
Does hipec improve outcomes in gastric cancer patients treated with perioperative chemotherapy and radical surgery? A propensity-score matched analysis.J Surg Oncol. 2020 Apr;121(5):823-832. doi: 10.1002/jso.25823. Epub 2020 Jan 16. J Surg Oncol. 2020. PMID: 31950511
-
[Neoadjuvant chemoradiotherapy combined with surgery versus direct surgery in the treatment of Siewert type II and III adenocarcinomas of the esophagogastric junction: long-term prognostic analysis of a prospective randomized controlled trial].Zhonghua Wei Chang Wai Ke Za Zhi. 2021 Feb 25;24(2):128-137. doi: 10.3760/cma.j.cn.441530-20201019-00565. Zhonghua Wei Chang Wai Ke Za Zhi. 2021. PMID: 33508918 Clinical Trial. Chinese.
-
Perioperative outcomes and survival in elderly patients aged ≥ 75 years undergoing gastrectomy for gastric cancer: an 18-year retrospective analysis in a single Western centre.Langenbecks Arch Surg. 2021 Jun;406(4):1057-1069. doi: 10.1007/s00423-021-02116-w. Epub 2021 Mar 26. Langenbecks Arch Surg. 2021. PMID: 33770264
-
[Safety and effectiveness of oxaliplatin combined with capecitabine or oxaliplatin combined with S-1 neoadjuvant chemotherapy in the treatment of advanced gastric cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2021 Feb 25;24(2):138-144. doi: 10.3760/cma.j.cn.441530-20200721-00433. Zhonghua Wei Chang Wai Ke Za Zhi. 2021. PMID: 33508919 Chinese.
-
[A multi-center retrospective study of perioperative chemotherapy for gastric cancer based on real-world data].Zhonghua Wei Chang Wai Ke Za Zhi. 2021 May 25;24(5):403-412. doi: 10.3760/cma.j.cn.441530-20200111-00014. Zhonghua Wei Chang Wai Ke Za Zhi. 2021. PMID: 34000769 Chinese.
Cited by
-
Anatomical and Biological Considerations to Determine Resectability in Pancreatic Cancer.Cancers (Basel). 2024 Jan 23;16(3):489. doi: 10.3390/cancers16030489. Cancers (Basel). 2024. PMID: 38339242 Free PMC article. Review.
-
Distinct characteristics of distant metastasis in early-onset gastric cancer patients compared to late-onset patients: An observational study.Medicine (Baltimore). 2024 May 17;103(20):e38098. doi: 10.1097/MD.0000000000038098. Medicine (Baltimore). 2024. PMID: 38758891 Free PMC article.
-
Definition and Predictors of Early Recurrence in Neoadjuvantly Treated Esophageal and Gastroesophageal Adenocarcinoma: a Dual-Center Retrospective Cohort Study.Ann Surg Oncol. 2025 Mar;32(3):1617-1627. doi: 10.1245/s10434-024-16403-5. Epub 2024 Nov 5. Ann Surg Oncol. 2025. PMID: 39499362 Free PMC article.
-
Early onset gastric cancer: clinical and molecular insights into a rising epidemic among younger adults.Proc (Bayl Univ Med Cent). 2025 Apr 22;38(4):388-396. doi: 10.1080/08998280.2025.2488592. eCollection 2025. Proc (Bayl Univ Med Cent). 2025. PMID: 40557205 Free PMC article.
-
Risk factors and nomogram development for lymph node metastasis in early-onset early-stage gastric cancer: a retrospective cohort study.Front Oncol. 2025 Apr 30;15:1544758. doi: 10.3389/fonc.2025.1544758. eCollection 2025. Front Oncol. 2025. PMID: 40371226 Free PMC article.
References
-
- Smyth EC, Nilsson M, Grabsch HI, van Grieken NC, Lordick F. Gastric cancer. Lancet. 2020;396:635–48. - PubMed
-
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M. et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–86. - PubMed
-
- Group. USCSW. U.S. Cancer Statistics Data Visualizations Tool, based on 2021 submission data (1999-2019). US Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute; wwwcdcgov/cancer/dataviz. 2022.
-
- Collaborative R, Zaborowski AM, Abdile A, Adamina M, Aigner F, d'Allens L. et al. Characteristics of Early-Onset vs Late-Onset Colorectal Cancer: A Review. JAMA Surg. 2021;156:865–74. - PubMed
-
- Kulig P, Nowakowski P, Sierzega M, Pach R, Majewska O, Markiewicz A. et al. Analysis of Prognostic Factors Affecting Short-term and Long-term Outcomes of Gastric Cancer Resection. Anticancer Res. 2021;41:3523–34. - PubMed
LinkOut - more resources
Full Text Sources
Medical
