

Extracellular Vesicle-Associated TWEAK Contributes to Vascular Inflammation and Remodeling During Acute Cellular Rejection
- PMID: 37325400
- PMCID: PMC10264567
- DOI: 10.1016/j.jacbts.2022.09.014
Extracellular Vesicle-Associated TWEAK Contributes to Vascular Inflammation and Remodeling During Acute Cellular Rejection
Abstract
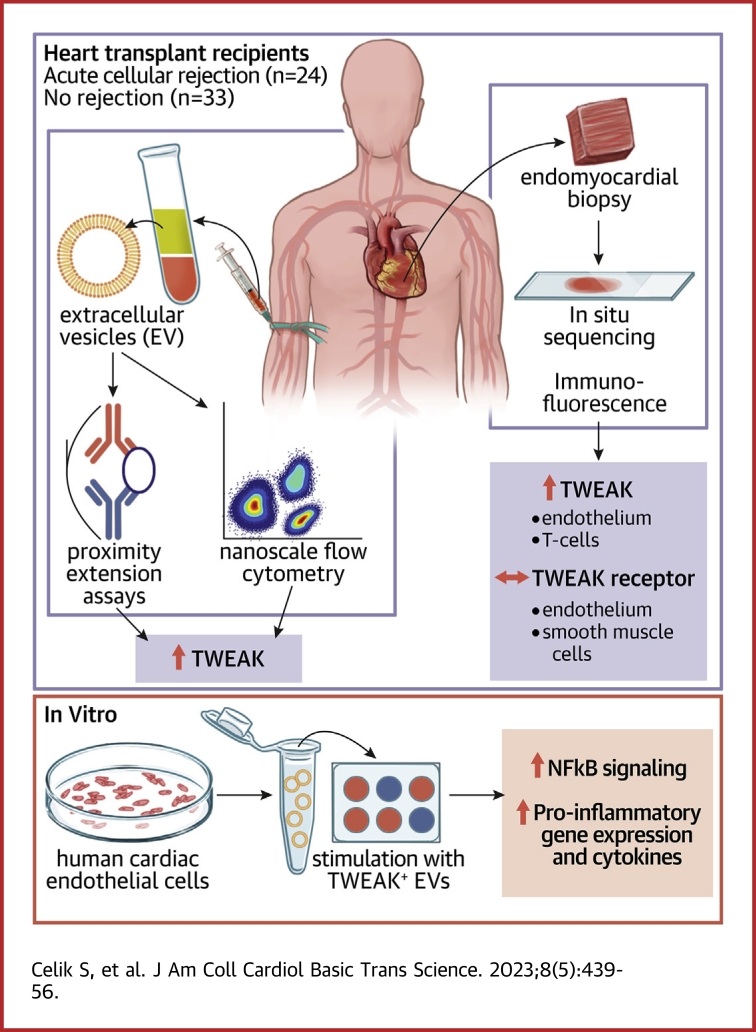
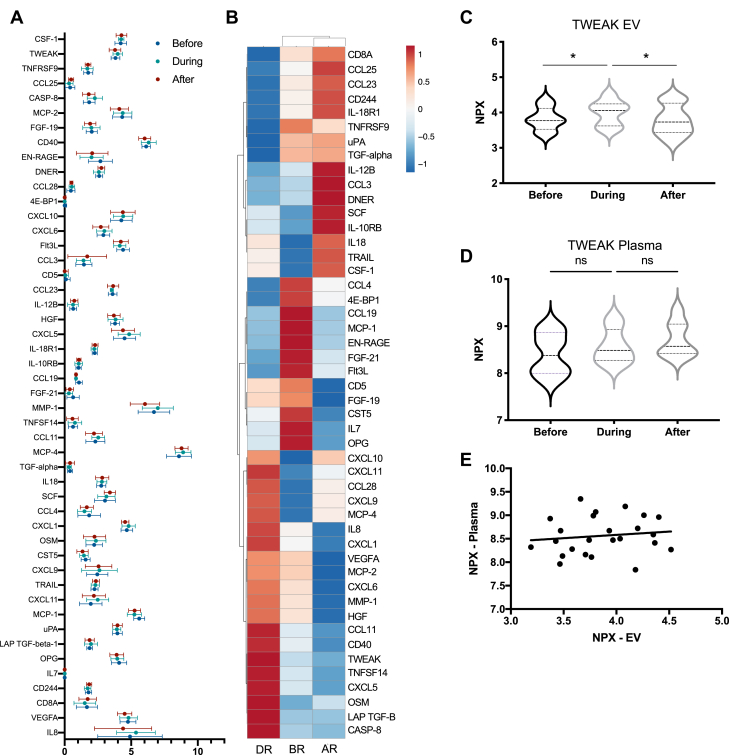
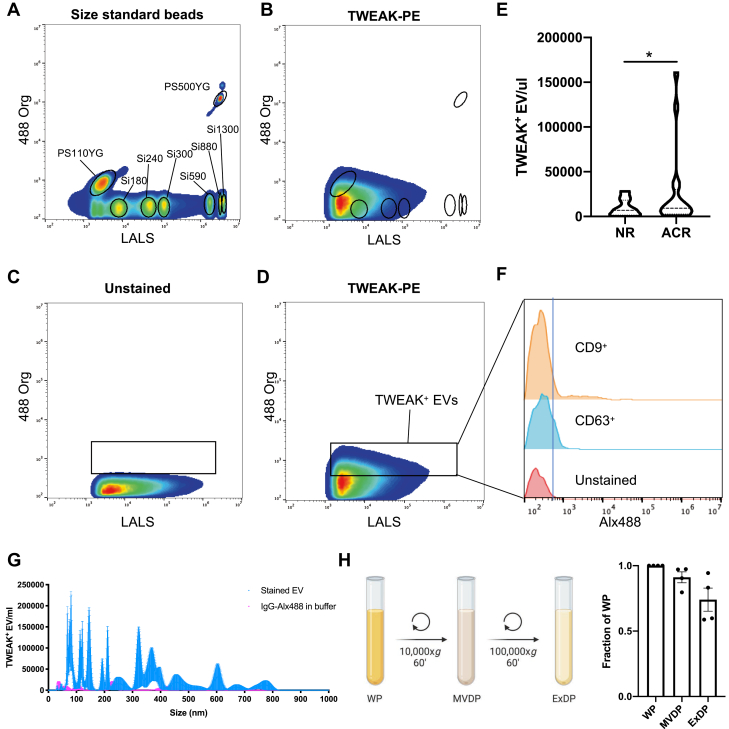
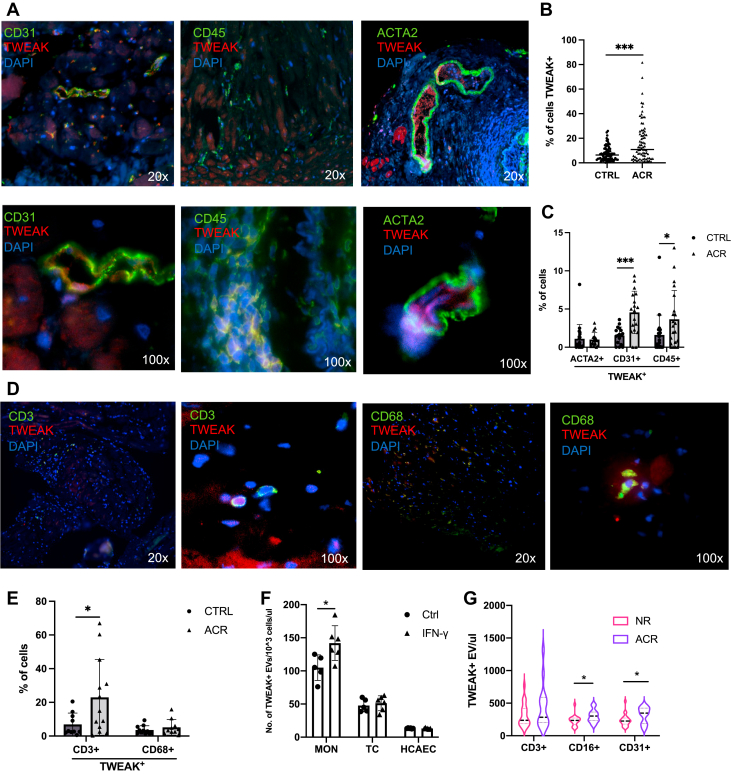
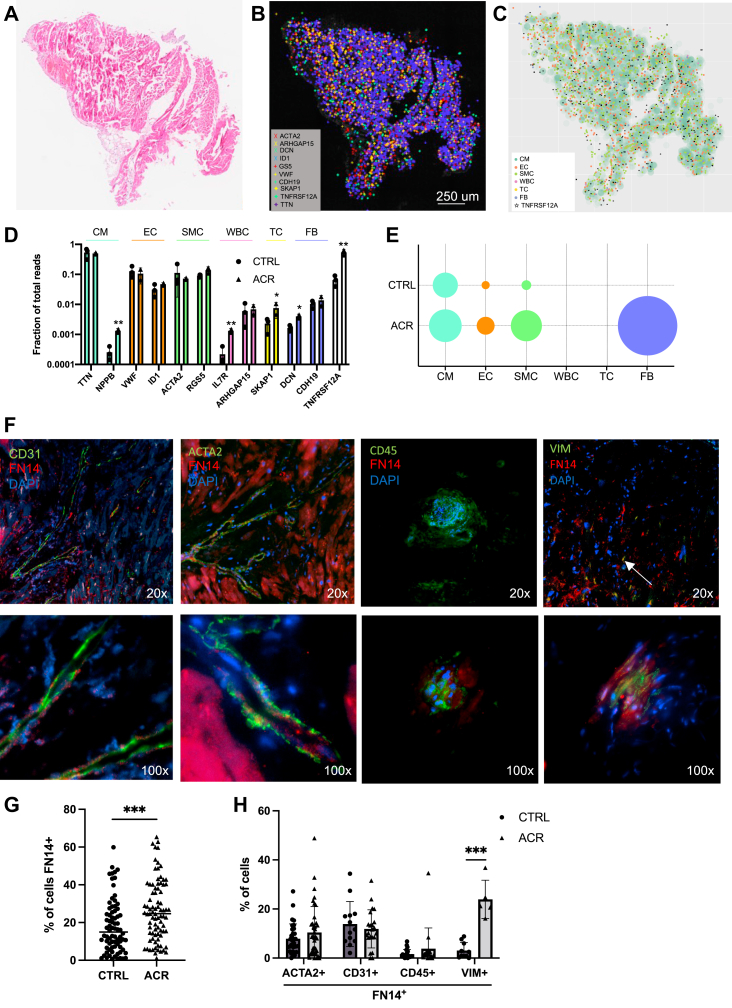
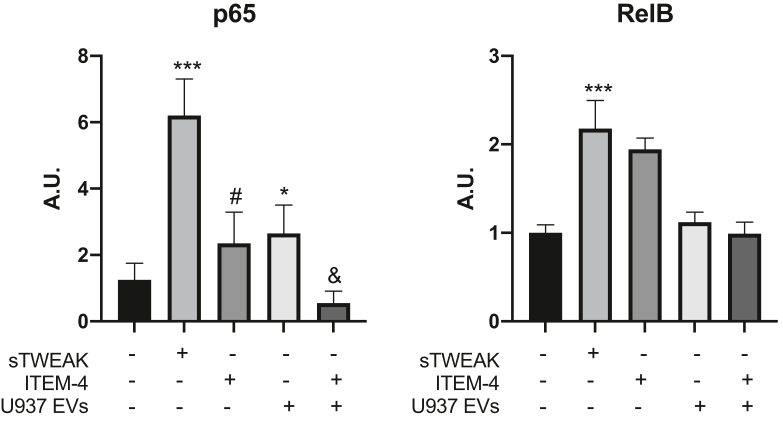
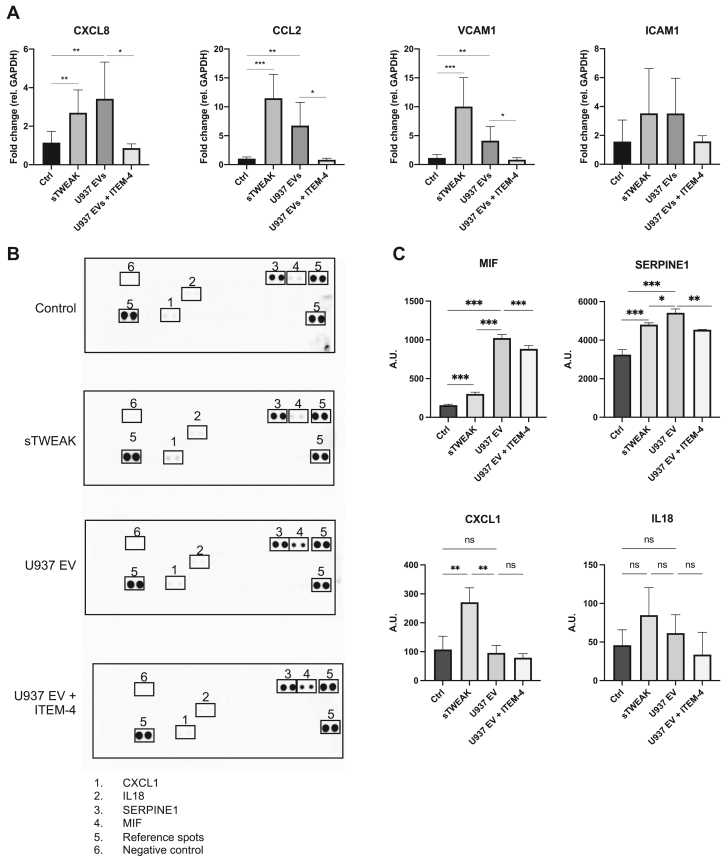
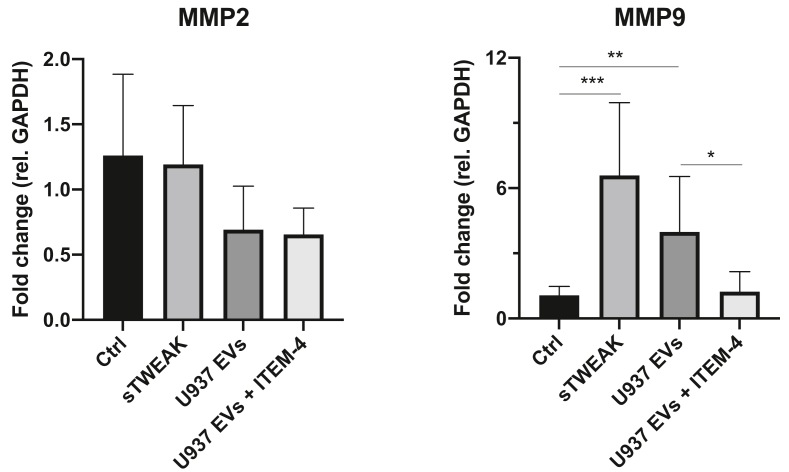
Acute cellular rejection (ACR) is a leading cause of graft loss and death after heart transplantation despite effective immunosuppressive therapies. The identification of factors that impair graft vascular barrier function or promote immune cell recruitment during ACR could provide new therapeutic opportunities for the treatment of patients who receive transplants. In 2 ACR cohorts, we found the extracellular vesicle-associated cytokine TWEAK to be elevated during ACR. Vesicular TWEAK promoted expression of proinflammatory genes and the release of chemoattractant cytokines from human cardiac endothelial cells. We conclude that vesicular TWEAK is a novel target with potential therapeutic implications in ACR.
Keywords: TWEAK; acute cellular rejection; chronic rejection; extracellular vesicle.
© 2023 The Authors.
Conflict of interest statement
Dr Smith was supported by grants from the Swedish Heart-Lung Foundation (2019-0526), the Swedish Research Council (2021-02273), the European Research Council (ERC-STG-2015-679242), Skåne University Hospital, governmental funding of clinical research within the Swedish National Health Service, a generous donation from the Knut and Alice Wallenberg Foundation to the Wallenberg Center for Molecular Medicine in Lund, and funding from the Swedish Research Council (Linnaeus grant Dnr 349-2006-237, Strategic Research Area Exodiab Dnr 2009-1039) and Swedish Foundation for Strategic Research (Dnr IRC15-0067) to the Lund University Diabetes Center. Dr Gidlöf is supported by the Swedish Heart and Lung Foundation (2020-0532), the Crafoord Foundation, the Magnus Bergvall Foundation, the Åke Wiberg Foundation, the Royal Physiographic Society and the Maggie Stephens Foundation. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Similar articles
-
IFN-γ-producing Th1-like regulatory T cells may limit acute cellular renal allograft rejection: Paradoxical post-transplantation effects of IFN-γ.Immunobiology. 2017 Feb;222(2):280-290. doi: 10.1016/j.imbio.2016.09.012. Epub 2016 Sep 19. Immunobiology. 2017. PMID: 27665996
-
The severity of acute cellular rejection defined by Banff classification is associated with kidney allograft outcomes.Transplantation. 2014 Jun 15;97(11):1146-54. doi: 10.1097/01.TP.0000441094.32217.05. Transplantation. 2014. PMID: 24892962
-
A Peripheral Blood Gene Expression Signature to Diagnose Subclinical Acute Rejection.J Am Soc Nephrol. 2019 Aug;30(8):1481-1494. doi: 10.1681/ASN.2018111098. Epub 2019 Jul 5. J Am Soc Nephrol. 2019. PMID: 31278196 Free PMC article.
-
Acute and Chronic Rejection After Liver Transplantation: What A Clinician Needs to Know.J Clin Exp Hepatol. 2017 Dec;7(4):358-366. doi: 10.1016/j.jceh.2017.10.003. Epub 2017 Nov 7. J Clin Exp Hepatol. 2017. PMID: 29234201 Free PMC article. Review.
-
Considering TWEAK as a target for therapy in renal and vascular injury.Cytokine Growth Factor Rev. 2009 Jun;20(3):251-8. doi: 10.1016/j.cytogfr.2009.05.002. Epub 2009 May 30. Cytokine Growth Factor Rev. 2009. PMID: 19482507 Review.
Cited by
-
Circulating extracellular vesicles as biomarkers in the diagnosis, prognosis and therapy of cardiovascular diseases.Front Cardiovasc Med. 2024 Sep 2;11:1425159. doi: 10.3389/fcvm.2024.1425159. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 39314768 Free PMC article. Review.
-
Extracellular Vesicles and Immune Activation in Solid Organ Transplantation: The Impact of Immunosuppression.BioDrugs. 2025 May;39(3):445-459. doi: 10.1007/s40259-025-00713-5. Epub 2025 Mar 26. BioDrugs. 2025. PMID: 40140222 Free PMC article. Review.
-
Extracellular Vesicles as Bridges Between Host Immune Cells and Graft Organ During Cellular Rejection.JACC Basic Transl Sci. 2023 May 22;8(5):457-459. doi: 10.1016/j.jacbts.2023.01.015. eCollection 2023 May. JACC Basic Transl Sci. 2023. PMID: 37325403 Free PMC article.
References
-
- Taylor D.O., Edwards L.B., Aurora P., et al. Registry of the International Society for Heart and Lung Transplantation: twenty-fifth official adult heart transplant report—2008. J Heart Lung Transplant. 2008;27:943–956. - PubMed
-
- Lund L.H., Khush K.K., Cherikh W.S., et al. The registry of the International Society for Heart and Lung Transplantation: thirty-fourth adult heart transplantation report—2017; focus theme: allograft ischemic time. J Heart Lung Transplant. 2017;36:1037–1046. - PubMed
-
- Raichlin E., Edwards B.S., Kremers W.K., et al. Acute cellular rejection and the subsequent development of allograft vasculopathy after cardiac transplantation. J Heart Lung Transplant. 2009;28:320–327. - PubMed
-
- Sato T., Seguchi O., Ishibashi-Ueda H., et al. Risk stratification for cardiac allograft vasculopathy in heart transplant recipients—annual intravascular ultrasound evaluation. Circ J. 2016;80:395–403. - PubMed
LinkOut - more resources
Full Text Sources
