

Comparison of CT-guided thoracic sympathetic nerve block and radiofrequency in the treatment of primary palmar hyperhidrosis
- PMID: 37325414
- PMCID: PMC10264635
- DOI: 10.3389/fsurg.2023.1126596
Comparison of CT-guided thoracic sympathetic nerve block and radiofrequency in the treatment of primary palmar hyperhidrosis
Abstract
Background: Primary palmar hyperhidrosis (PPH) is a condition marked by an overactive secretion of the hand's exocrine glands and is frequently hereditary. The profuse sweating associated with this condition can significantly impair the patient's daily activities and quality of life.
Objective: The objective of this study was to compared the benefits and drawbacks of thoracic sympathetic block and thoracic sympathetic radiofrequency in the treatment of PPH.
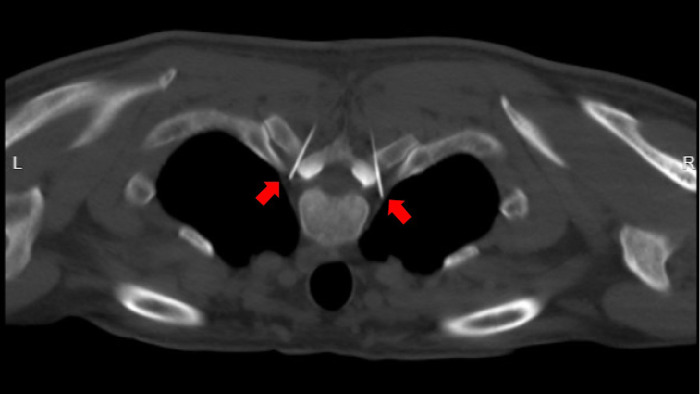
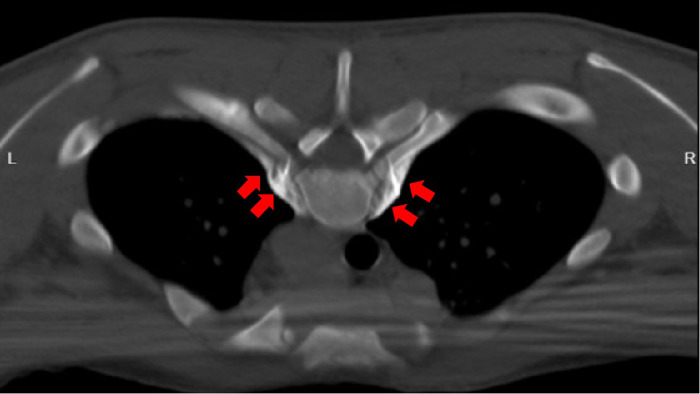
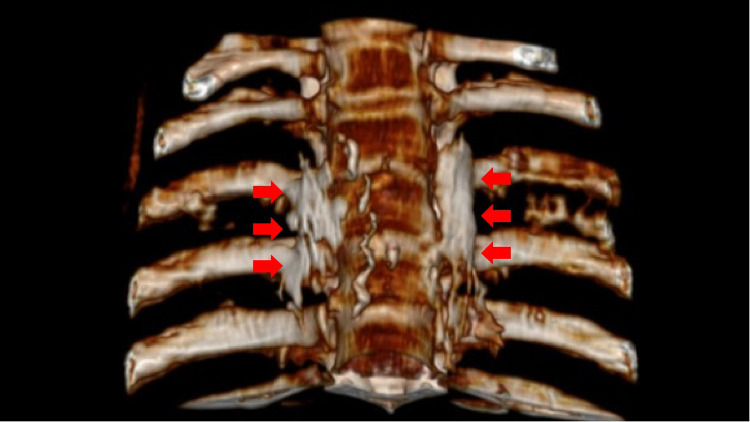
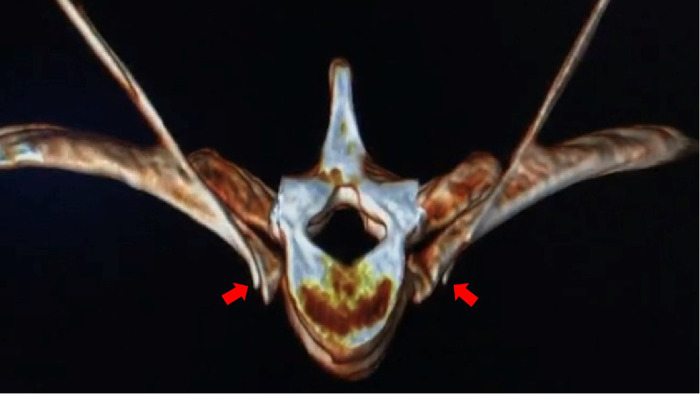
Methods: A retrospective analysis was conducted on 69 patients. They were divided into groups A and B according to their treatment. Group A (34 cases) received CT-guided percutaneous thoracic sympathetic nerve chain anhydrous alcohol chemical damage block, and group B (35 cases) received CT-guided percutaneous thoracic sympathetic nerve chain radiofrequency thermocoagulation.
Results: Palmar sweating disappeared immediately after the operation. The recurrence rates at 1, 3, 6, 12, 24, and 36 months were 5.88% vs. 2.86% (P > 0.05), 20.59% vs. 5.71% (P > 0.05), 32.35% vs. 11.43% (P < 0.05),32.35% vs. 11.43% (P < 0.05), 25% vs. 14.71% (P < 0.05), and 68.75% vs. 20.59% (P < 0.05), respectively. The incidence of intercostal neuralgia and compensatory hyperhidrosis was higher in group A compared with of group B (52.94% vs. 22.86%, P < 0.05; 55.88% vs. 22.86%, P < 0.05).
Conclusion: Both methods were found to be effective in treating PPH, but thoracic sympathetic radiofrequency had a longer-term effect, a lower recurrence rate, and a lower incidence of intercostal neuralgia and compensatory hyperhidrosis than a thoracic sympathetic block.
Keywords: autonomic nerve block; hyperhidrosis; nerve block; palmar; radiofrequency therapy; sympathetic.
© 2023 Zhang, Xu, Liu, Zhao, Ma and Haung.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Advances in the Treatment of Neuropathic Pain by Sympathetic Regulation.Curr Pain Headache Rep. 2024 Nov;28(11):1167-1176. doi: 10.1007/s11916-024-01285-9. Epub 2024 Jun 22. Curr Pain Headache Rep. 2024. PMID: 38907791 Free PMC article. Review.
-
Risk Factors Affecting the Outcomes of CT-Guided Radiofrequency Thermocoagulation of Thoracic Sympathetic Nerve in the Treatment of Primary Palm Hyperhidrosis.Pain Physician. 2022 Nov;25(8):E1219-E1228. Pain Physician. 2022. PMID: 36375194
-
[Therapeutic feasibility of percutaneous puncture and chemical neurolysis of thoracic sympathetic nerve block in palmar hyperhidrosis under the guidance of computed tomograph].Zhonghua Yi Xue Za Zhi. 2011 Oct 18;91(38):2710-3. Zhonghua Yi Xue Za Zhi. 2011. PMID: 22321983 Chinese.
-
Needlescopic Video-Assisted Thoracic Bilateral T4 Sympathicotomy for the Treatment of Primary Palmar Hyperhidrosis: An Analysis of 200 Cases.Thorac Cardiovasc Surg. 2019 Aug;67(5):395-401. doi: 10.1055/s-0038-1645872. Epub 2018 May 1. Thorac Cardiovasc Surg. 2019. PMID: 29715706
-
Limited endoscopic thoracic sympathetic block for hyperhidrosis of the upper limb: reduction of compensatory sweating by clipping T4.Surg Endosc. 2004 Jan;18(1):152-6. doi: 10.1007/s00464-002-8940-5. Epub 2003 Nov 21. Surg Endosc. 2004. PMID: 14625754 Review.
Cited by
-
Advances in the Treatment of Neuropathic Pain by Sympathetic Regulation.Curr Pain Headache Rep. 2024 Nov;28(11):1167-1176. doi: 10.1007/s11916-024-01285-9. Epub 2024 Jun 22. Curr Pain Headache Rep. 2024. PMID: 38907791 Free PMC article. Review.
References
-
- Xie H, Lu T, Zhu L, Zhu D, Wei T, Yuan G, et al. A retrospective cohort study of T3 versus T4 thoracoscopic sympathectomy for primary palmar hyperhidrosis and primary palmar hyperhidrosis with axillary and plantar sweating. Videosurgery Miniinv Techniques. (2020) 15(3):488–95. 10.5114/wiitm.2019.89656 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources