

Video versus Direct Laryngoscopy for Tracheal Intubation of Critically Ill Adults
- PMID: 37326325
- PMCID: PMC11075576
- DOI: 10.1056/NEJMoa2301601
Video versus Direct Laryngoscopy for Tracheal Intubation of Critically Ill Adults
Abstract
Background: Whether video laryngoscopy as compared with direct laryngoscopy increases the likelihood of successful tracheal intubation on the first attempt among critically ill adults is uncertain.
Methods: In a multicenter, randomized trial conducted at 17 emergency departments and intensive care units (ICUs), we randomly assigned critically ill adults undergoing tracheal intubation to the video-laryngoscope group or the direct-laryngoscope group. The primary outcome was successful intubation on the first attempt. The secondary outcome was the occurrence of severe complications during intubation; severe complications were defined as severe hypoxemia, severe hypotension, new or increased vasopressor use, cardiac arrest, or death.
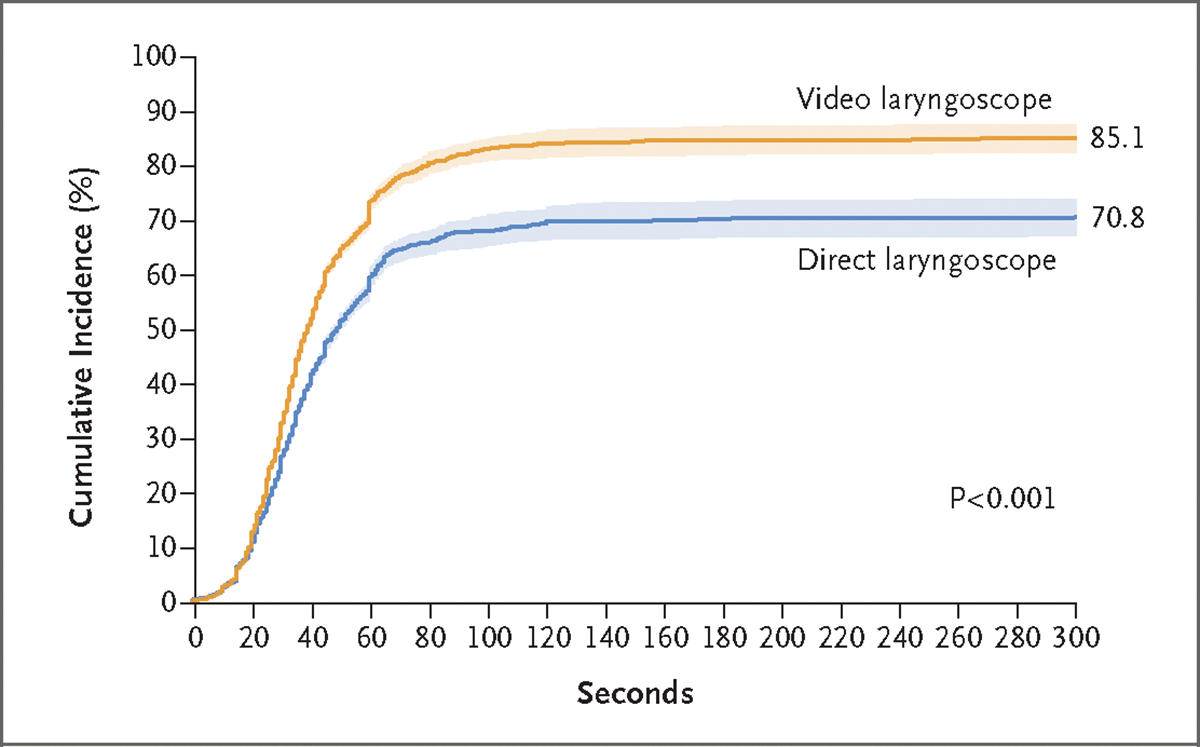
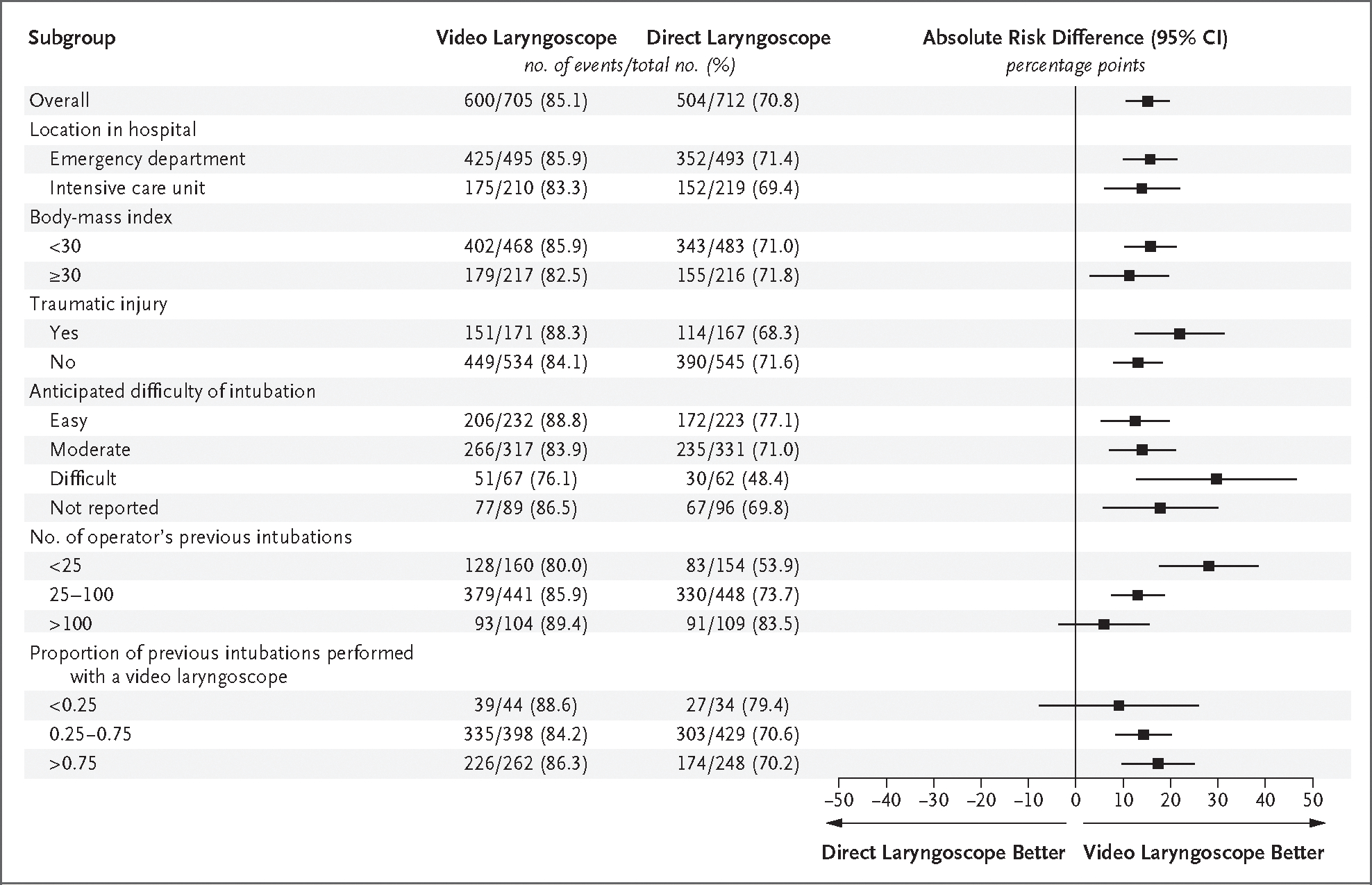
Results: The trial was stopped for efficacy at the time of the single preplanned interim analysis. Among 1417 patients who were included in the final analysis (91.5% of whom underwent intubation that was performed by an emergency medicine resident or a critical care fellow), successful intubation on the first attempt occurred in 600 of the 705 patients (85.1%) in the video-laryngoscope group and in 504 of the 712 patients (70.8%) in the direct-laryngoscope group (absolute risk difference, 14.3 percentage points; 95% confidence interval [CI], 9.9 to 18.7; P<0.001). A total of 151 patients (21.4%) in the video-laryngoscope group and 149 patients (20.9%) in the direct-laryngoscope group had a severe complication during intubation (absolute risk difference, 0.5 percentage points; 95% CI, -3.9 to 4.9). Safety outcomes, including esophageal intubation, injury to the teeth, and aspiration, were similar in the two groups.
Conclusions: Among critically ill adults undergoing tracheal intubation in an emergency department or ICU, the use of a video laryngoscope resulted in a higher incidence of successful intubation on the first attempt than the use of a direct laryngoscope. (Funded by the U.S. Department of Defense; DEVICE ClinicalTrials.gov number, NCT05239195.).
Copyright © 2023 Massachusetts Medical Society.
Figures
Comment in
-
Video versus direct laryngoscopy for tracheal intubation of critically ill adults.CJEM. 2024 May;26(5):319-320. doi: 10.1007/s43678-024-00683-7. Epub 2024 Apr 1. CJEM. 2024. PMID: 38558294 No abstract available.
References
-
- Pfuntner A, Wier LM, Stocks C. Most frequent procedures performed in U.S. hospitals, 2011. Rockville, MD: Agency for Healthcare Research and Quality, October 2013 (https://www.ncbi.nlm.nih.gov/books/NBK174682/pdf/Bookshelf_NBK174682.pdf). - PubMed
-
- Cairns C, Kang K, Santo L. National Hospital Ambulatory Medical Care Survey: 2018 emergency department summary tables. Washington, DC: National Center for Health Statistics; (https://www.cdc.gov/nchs/data/nhamcs/web_tables/2018-ed-web-tables-508.pdf).
-
- Mort TC. Emergency tracheal intubation: complications associated with repeated laryngoscopic attempts. Anesth Analg 2004;99:6 07–13. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical