

Small molecules restore azole activity against drug-tolerant and drug-resistant Candida isolates
- PMID: 37326546
- PMCID: PMC10470600
- DOI: 10.1128/mbio.00479-23
Small molecules restore azole activity against drug-tolerant and drug-resistant Candida isolates
Abstract
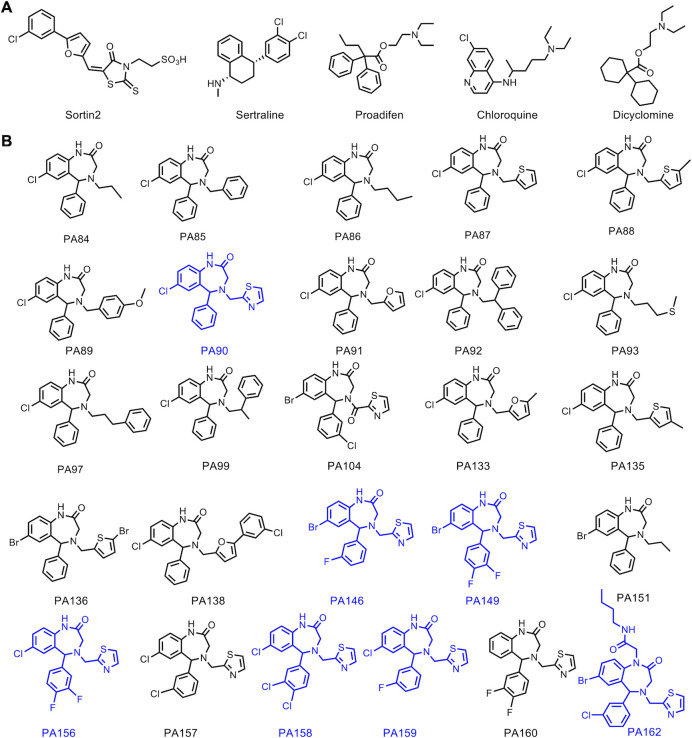
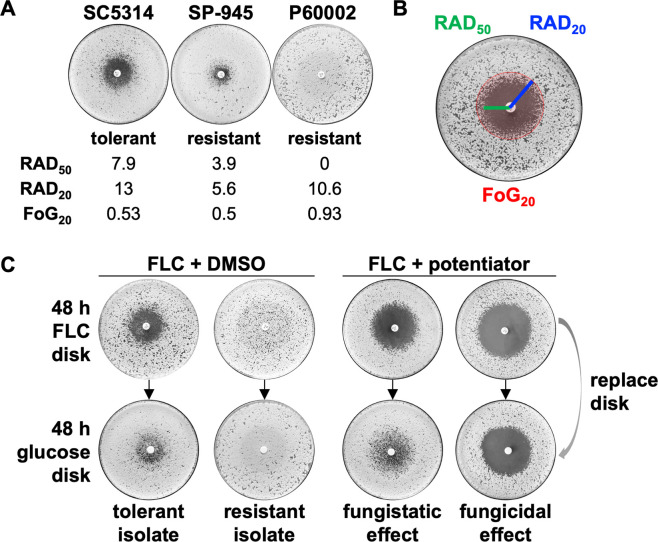
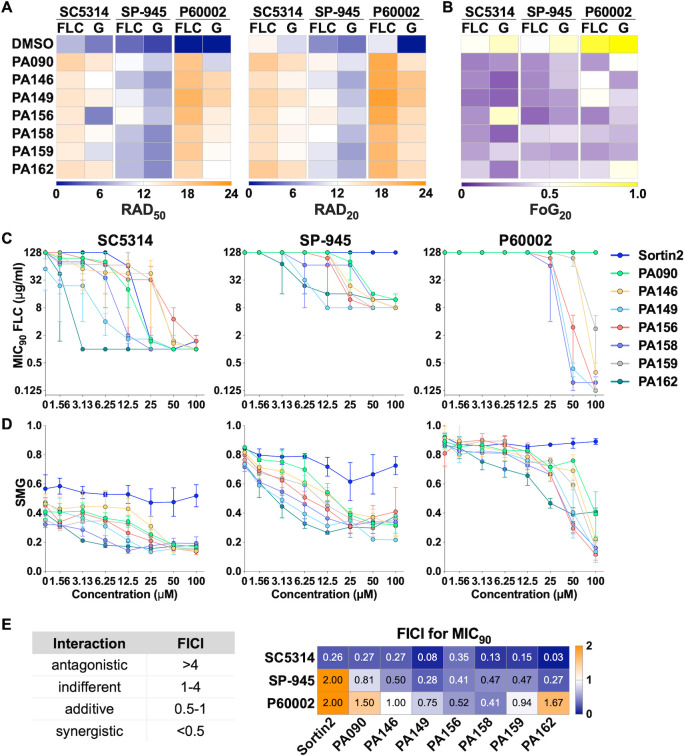
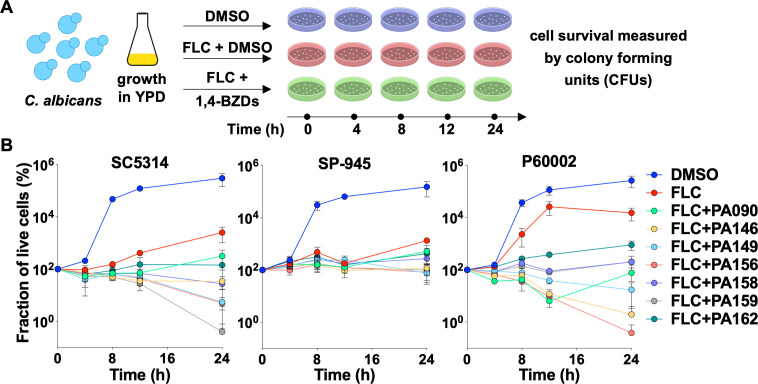
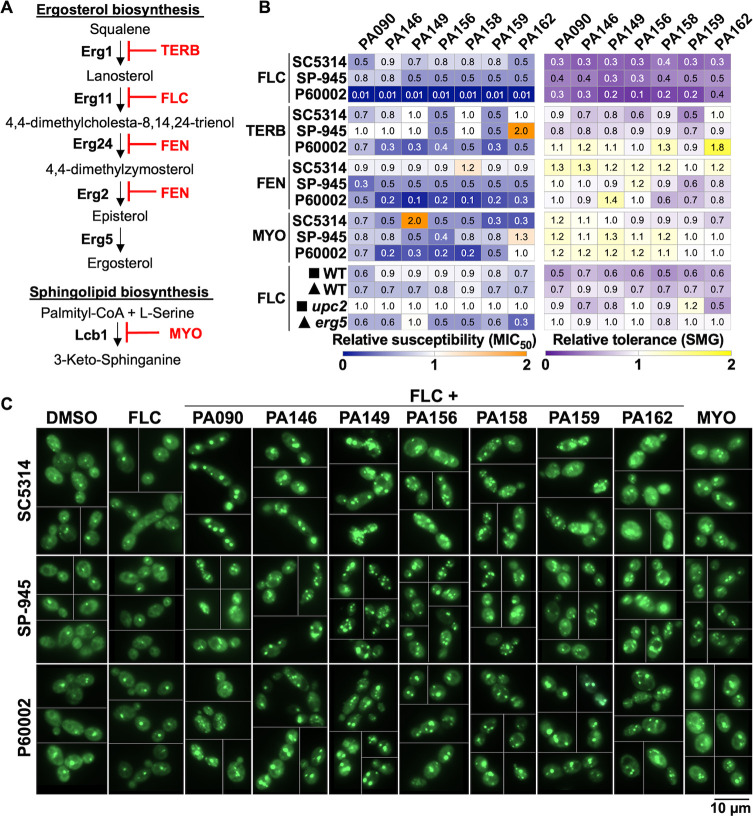
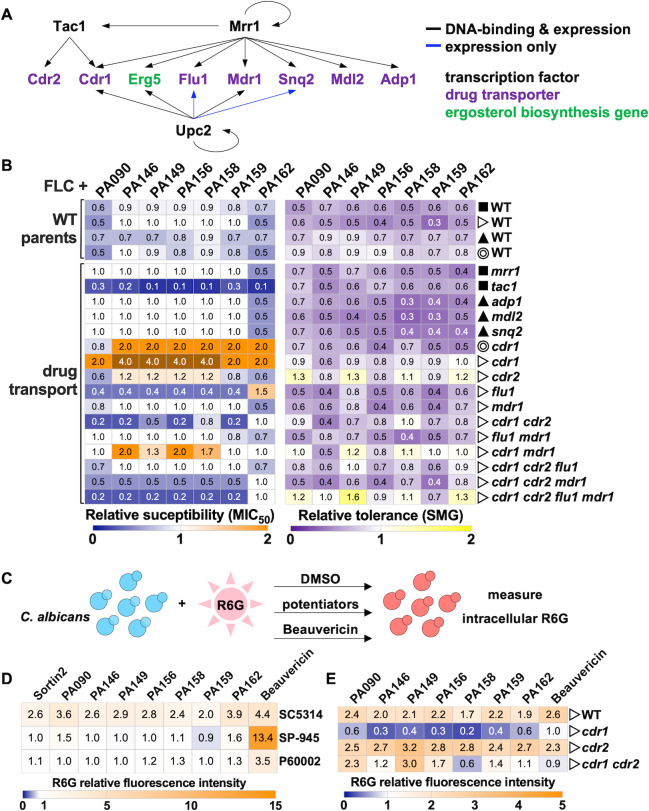
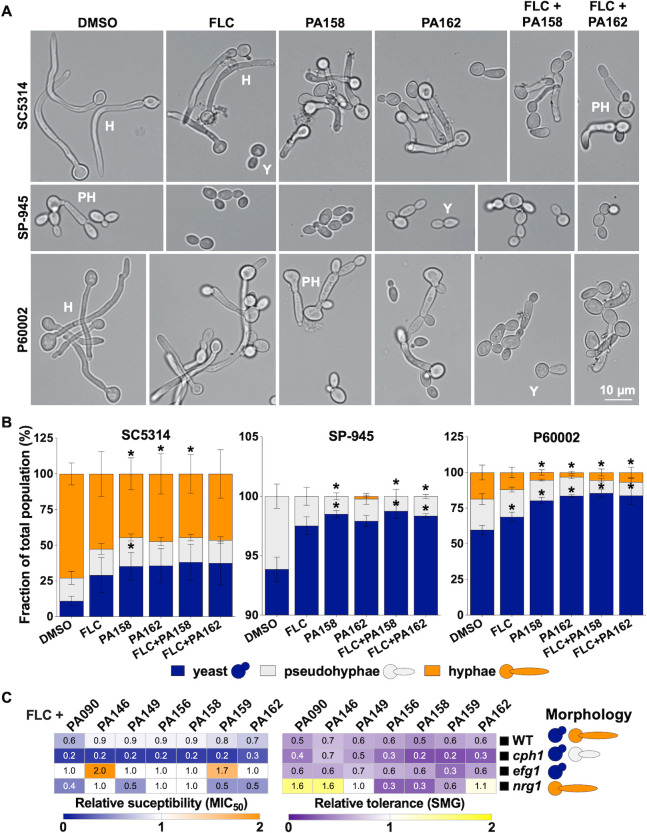
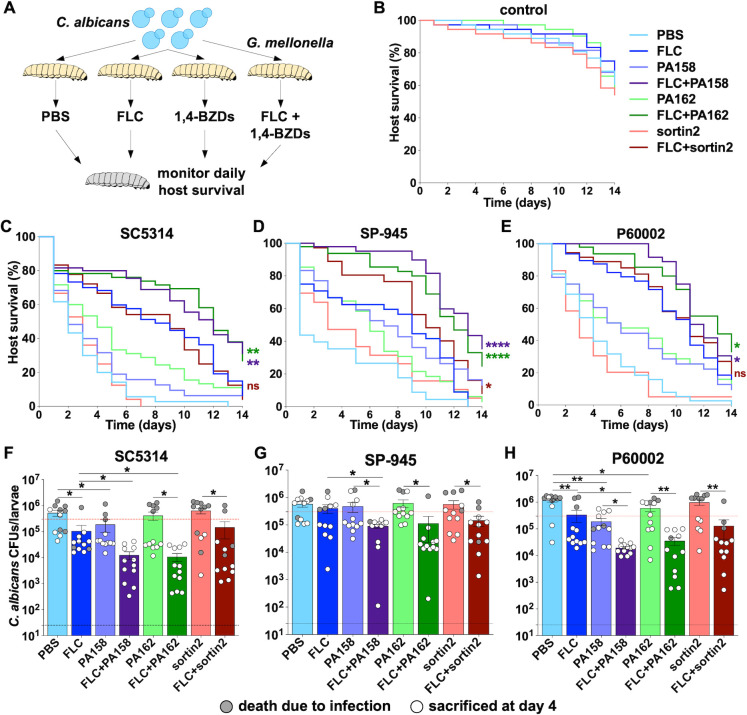
Each year, fungi cause more than 1.5 billion infections worldwide and have a devastating impact on human health, particularly in immunocompromised individuals or patients in intensive care units. The limited antifungal arsenal and emerging multidrug-resistant species necessitate the development of new therapies. One strategy for combating drug-resistant pathogens is the administration of molecules that restore fungal susceptibility to approved drugs. Accordingly, we carried out a screen to identify small molecules that could restore the susceptibility of pathogenic Candida species to azole antifungals. This screening effort led to the discovery of novel 1,4-benzodiazepines that restore fluconazole susceptibility in resistant isolates of Candida albicans, as evidenced by 100-1,000-fold potentiation of fluconazole activity. This potentiation effect was also observed in azole-tolerant strains of C. albicans and in other pathogenic Candida species. The 1,4-benzodiazepines selectively potentiated different azoles, but not other approved antifungals. A remarkable feature of the potentiation was that the combination of the compounds with fluconazole was fungicidal, whereas fluconazole alone is fungistatic. Interestingly, the potentiators were not toxic to C. albicans in the absence of fluconazole, but inhibited virulence-associated filamentation of the fungus. We found that the combination of the potentiators and fluconazole significantly enhanced host survival in a Galleria mellonella model of systemic fungal infection. Taken together, these observations validate a strategy wherein small molecules can restore the activity of highly used anti-infectives that have lost potency. IMPORTANCE In the last decade, we have been witnessing a higher incidence of fungal infections, due to an expansion of the fungal species capable of causing disease (e.g., Candida auris), as well as increased antifungal drug resistance. Among human fungal pathogens, Candida species are a leading cause of invasive infections and are associated with high mortality rates. Infections by these pathogens are commonly treated with azole antifungals, yet the expansion of drug-resistant isolates has reduced their clinical utility. In this work, we describe the discovery and characterization of small molecules that potentiate fluconazole and restore the susceptibility of azole-resistant and azole-tolerant Candida isolates. Interestingly, the potentiating 1,4-benzodiazepines were not toxic to fungal cells but inhibited their virulence-associated filamentous growth. Furthermore, combinations of the potentiators and fluconazole decreased fungal burdens and enhanced host survival in a Galleria mellonella model of systemic fungal infections. Accordingly, we propose the use of novel antifungal potentiators as a powerful strategy for addressing the growing resistance of fungi to clinically approved drugs.
Keywords: 1,4-benzodiazepines; Candida albicans; azole resistance; azole tolerance; drug combinations.
Conflict of interest statement
The authors declare no conflict of interest
Figures
Comment in
-
Powering up antifungal treatment: using small molecules to unlock the potential of existing therapies.mBio. 2023 Aug 31;14(4):e0107323. doi: 10.1128/mbio.01073-23. Epub 2023 Aug 2. mBio. 2023. PMID: 37530533 Free PMC article.
Similar articles
-
Resistance in human pathogenic yeasts and filamentous fungi: prevalence, underlying molecular mechanisms and link to the use of antifungals in humans and the environment.Dan Med J. 2016 Oct;63(10):B5288. Dan Med J. 2016. PMID: 27697142 Review.
-
Oxadiazole-Containing Macrocyclic Peptides Potentiate Azole Activity against Pathogenic Candida Species.mSphere. 2020 Apr 8;5(2):e00256-20. doi: 10.1128/mSphere.00256-20. mSphere. 2020. PMID: 32269162 Free PMC article.
-
Candida and candidaemia. Susceptibility and epidemiology.Dan Med J. 2013 Nov;60(11):B4698. Dan Med J. 2013. PMID: 24192246 Review.
-
Spectrum of activity and mechanisms of azole-bisphosphonate synergy in pathogenic Candida.Microbiol Spectr. 2024 Jun 4;12(6):e0012124. doi: 10.1128/spectrum.00121-24. Epub 2024 May 2. Microbiol Spectr. 2024. PMID: 38695556 Free PMC article.
-
In Vitro and In Vivo Interactions of TOR Inhibitor AZD8055 and Azoles against Pathogenic Fungi.Microbiol Spectr. 2022 Feb 23;10(1):e0200721. doi: 10.1128/spectrum.02007-21. Epub 2022 Jan 12. Microbiol Spectr. 2022. PMID: 35019705 Free PMC article.
Cited by
-
Surfactin and Capric Acid Affect the Posaconazole Susceptibility of Candida albicans Strains with Altered Sterols and Sphingolipids Biosynthesis.Int J Mol Sci. 2023 Dec 15;24(24):17499. doi: 10.3390/ijms242417499. Int J Mol Sci. 2023. PMID: 38139328 Free PMC article.
-
Anticandidal effect of cinnamic acid characterized from Cinnamomum cassia bark against the fluconazole resistant strains of Candida.Braz J Microbiol. 2024 Dec;55(4):3655-3666. doi: 10.1007/s42770-024-01469-w. Epub 2024 Jul 24. Braz J Microbiol. 2024. PMID: 39046694 Free PMC article.
-
Miconazole induces aneuploidy-mediated tolerance in Candida albicans that is dependent on Hsp90 and calcineurin.Front Cell Infect Microbiol. 2024 Jun 25;14:1392564. doi: 10.3389/fcimb.2024.1392564. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 38983116 Free PMC article.
-
Azole potentiation in Candida species.PLoS Pathog. 2023 Aug 31;19(8):e1011583. doi: 10.1371/journal.ppat.1011583. eCollection 2023 Aug. PLoS Pathog. 2023. PMID: 37651385 Free PMC article.
-
Approaches for identifying and measuring heteroresistance in azole-susceptible Candida isolates.Microbiol Spectr. 2024 Apr 2;12(4):e0404123. doi: 10.1128/spectrum.04041-23. Epub 2024 Mar 14. Microbiol Spectr. 2024. PMID: 38483474 Free PMC article.
References
-
- Kett DH, Azoulay E, Echeverria PM, Vincent J-L, Extended Prevalence of Infection in ICU Study (EPIC II) Group of Investigators . 2011. Candida bloodstream infections in intensive care units: analysis of the extended prevalence of infection in intensive care unit study. Crit Care Med 39:665–670. doi:10.1097/CCM.0b013e318206c1ca - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
