

Predicting chronic postsurgical pain: current evidence and a novel program to develop predictive biomarker signatures
- PMID: 37326643
- PMCID: PMC10436361
- DOI: 10.1097/j.pain.0000000000002938
Predicting chronic postsurgical pain: current evidence and a novel program to develop predictive biomarker signatures
Abstract
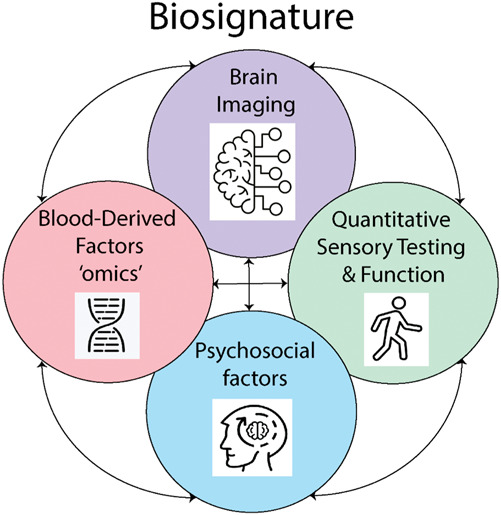
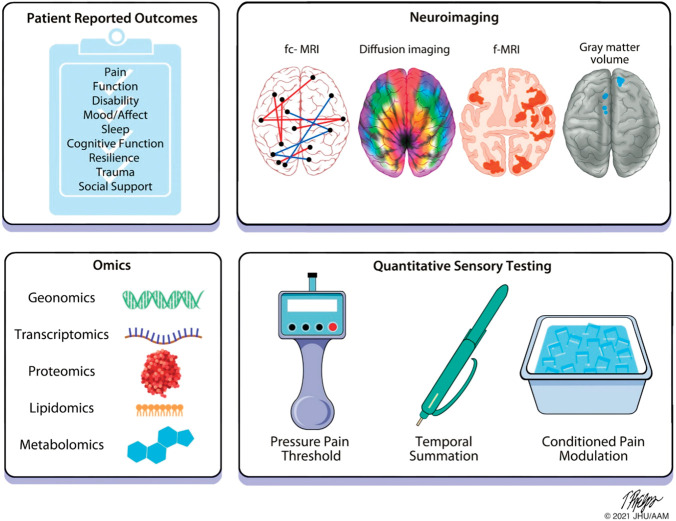
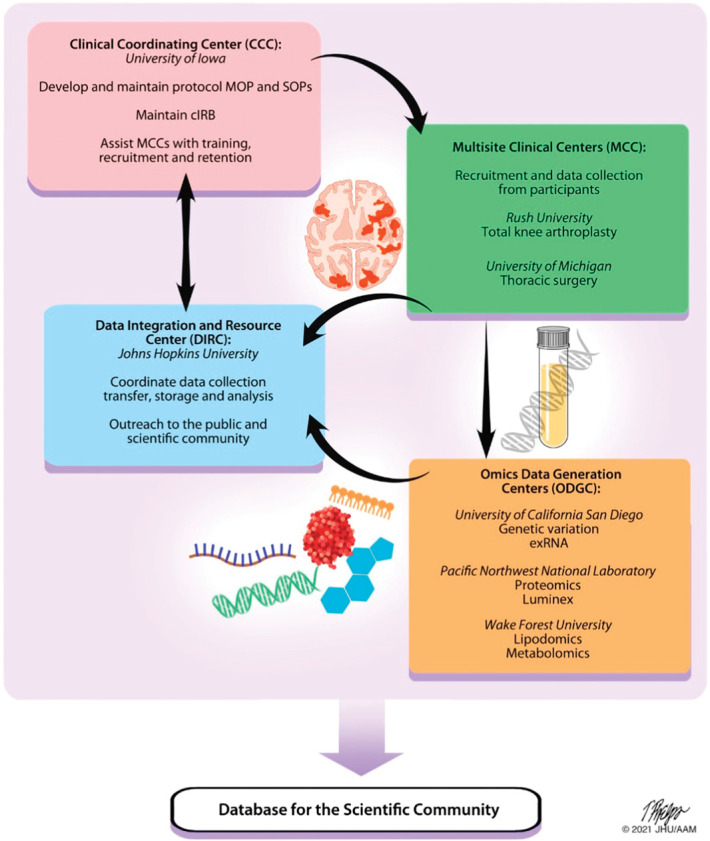
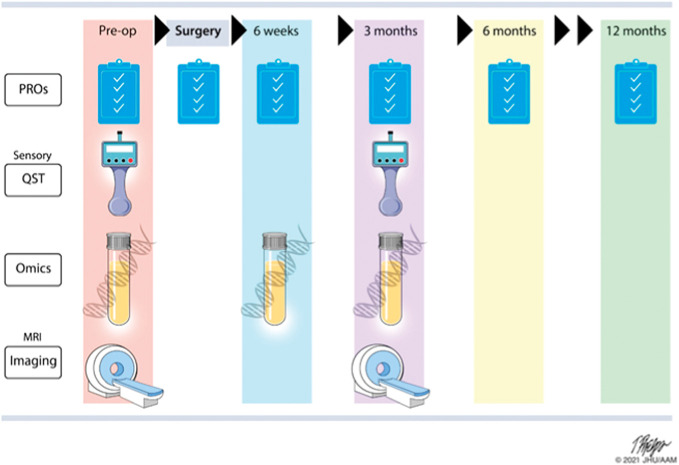
Chronic pain affects more than 50 million Americans. Treatments remain inadequate, in large part, because the pathophysiological mechanisms underlying the development of chronic pain remain poorly understood. Pain biomarkers could potentially identify and measure biological pathways and phenotypical expressions that are altered by pain, provide insight into biological treatment targets, and help identify at-risk patients who might benefit from early intervention. Biomarkers are used to diagnose, track, and treat other diseases, but no validated clinical biomarkers exist yet for chronic pain. To address this problem, the National Institutes of Health Common Fund launched the Acute to Chronic Pain Signatures (A2CPS) program to evaluate candidate biomarkers, develop them into biosignatures, and discover novel biomarkers for chronification of pain after surgery. This article discusses candidate biomarkers identified by A2CPS for evaluation, including genomic, proteomic, metabolomic, lipidomic, neuroimaging, psychophysical, psychological, and behavioral measures. Acute to Chronic Pain Signatures will provide the most comprehensive investigation of biomarkers for the transition to chronic postsurgical pain undertaken to date. Data and analytic resources generatedby A2CPS will be shared with the scientific community in hopes that other investigators will extract valuable insights beyond A2CPS's initial findings. This article will review the identified biomarkers and rationale for including them, the current state of the science on biomarkers of the transition from acute to chronic pain, gaps in the literature, and how A2CPS will address these gaps.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the International Association for the Study of Pain.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
References
-
- Althaus A, Arránz Becker O, Neugebauer E. Distinguishing between pain intensity and pain resolution: using acute post-surgical pain trajectories to predict chronic post-surgical pain. Eur J Pain 2014;18:513–21. - PubMed
-
- Antunes-Martins A, Perkins JR, Lees J, Hildebrandt T, Orengo C, Bennett DL. Systems biology approaches to finding novel pain mediators. Wiley Interdiscip Rev Syst Biol Med 2013;5:11–35. - PubMed
