

Trends in Use of Medication to Treat Opioid Use Disorder During the COVID-19 Pandemic in 10 State Medicaid Programs
- PMID: 37327009
- PMCID: PMC10276306
- DOI: 10.1001/jamahealthforum.2023.1422
Trends in Use of Medication to Treat Opioid Use Disorder During the COVID-19 Pandemic in 10 State Medicaid Programs
Abstract
Importance: Federal and state agencies granted temporary regulatory waivers to prevent disruptions in access to medication for opioid use disorder (MOUD) during the COVID-19 pandemic, including expanding access to telehealth for MOUD. Little is known about changes in MOUD receipt and initiation among Medicaid enrollees during the pandemic.
Objectives: To examine changes in receipt of any MOUD, initiation of MOUD (in-person vs telehealth), and the proportion of days covered (PDC) with MOUD after initiation from before to after declaration of the COVID-19 public health emergency (PHE).
Design, setting, and participants: This serial cross-sectional study included Medicaid enrollees aged 18 to 64 years in 10 states from May 2019 through December 2020. Analyses were conducted from January through March 2022.
Exposures: Ten months before the COVID-19 PHE (May 2019 through February 2020) vs 10 months after the PHE was declared (March through December 2020).
Main outcomes and measures: Primary outcomes included receipt of any MOUD and outpatient initiation of MOUD via prescriptions and office- or facility-based administrations. Secondary outcomes included in-person vs telehealth MOUD initiation and PDC with MOUD after initiation.
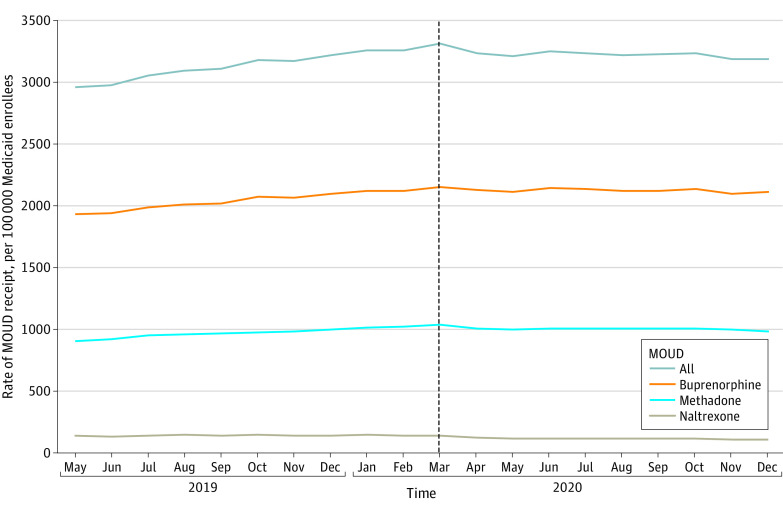
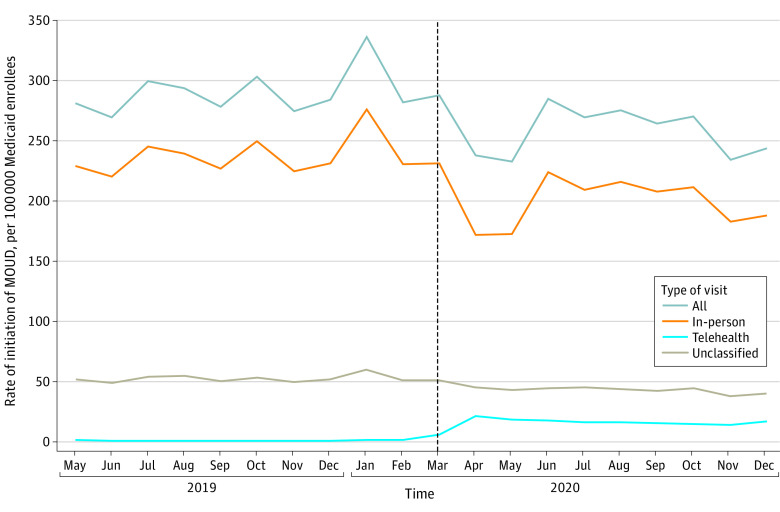
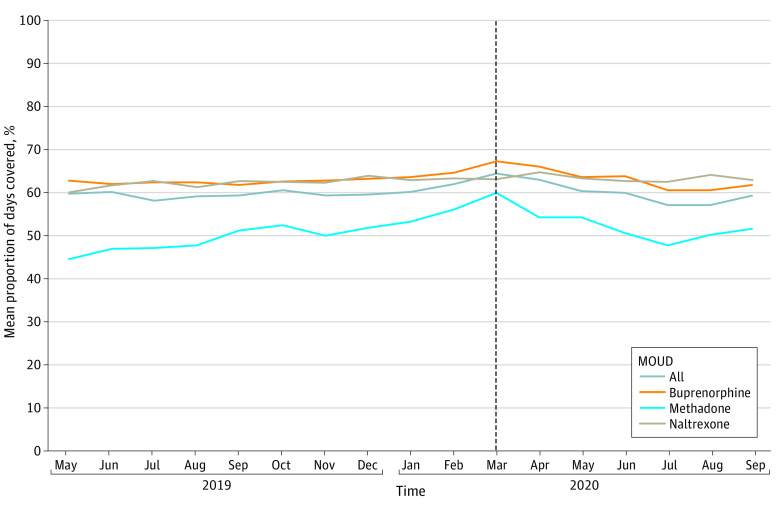
Results: Among a total of 8 167 497 Medicaid enrollees before the PHE and 8 181 144 after the PHE, 58.6% were female in both periods and most enrollees were aged 21 to 34 years (40.1% before the PHE; 40.7% after the PHE). Monthly rates of MOUD initiation, representing 7% to 10% of all MOUD receipt, decreased immediately after the PHE primarily due to reductions in in-person initiations (from 231.3 per 100 000 enrollees in March 2020 to 171.8 per 100 000 enrollees in April 2020) that were partially offset by increases in telehealth initiations (from 5.6 per 100 000 enrollees in March 2020 to 21.1 per 100 000 enrollees in April 2020). Mean monthly PDC with MOUD in the 90 days after initiation decreased after the PHE (from 64.5% in March 2020 to 59.5% in September 2020). In adjusted analyses, there was no immediate change (odds ratio [OR], 1.01; 95% CI, 1.00-1.01) or change in the trend (OR, 1.00; 95% CI, 1.00-1.01) in the likelihood of receipt of any MOUD after the PHE compared with before the PHE. There was an immediate decrease in the likelihood of outpatient MOUD initiation (OR, 0.90; 95% CI, 0.85-0.96) and no change in the trend in the likelihood of outpatient MOUD initiation (OR, 0.99; 95% CI, 0.98-1.00) after the PHE compared with before the PHE.
Conclusions and relevance: In this cross-sectional study of Medicaid enrollees, the likelihood of receipt of any MOUD was stable from May 2019 through December 2020 despite concerns about potential COVID-19 pandemic-related disruptions in care. However, immediately after the PHE was declared, there was a reduction in overall MOUD initiations, including a reduction in in-person MOUD initiations that was only partially offset by increased use of telehealth.
Conflict of interest statement
Figures
References
-
- Centers for Disease Control and Prevention . Provisional drug overdose death counts. Accessed May 3, 2023. https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
