

Patients' access to and acceptance of community-based hepatitis C testing and treatment in Myanmar: A mixed-method study
- PMID: 37327249
- PMCID: PMC10275420
- DOI: 10.1371/journal.pgph.0000902
Patients' access to and acceptance of community-based hepatitis C testing and treatment in Myanmar: A mixed-method study
Abstract
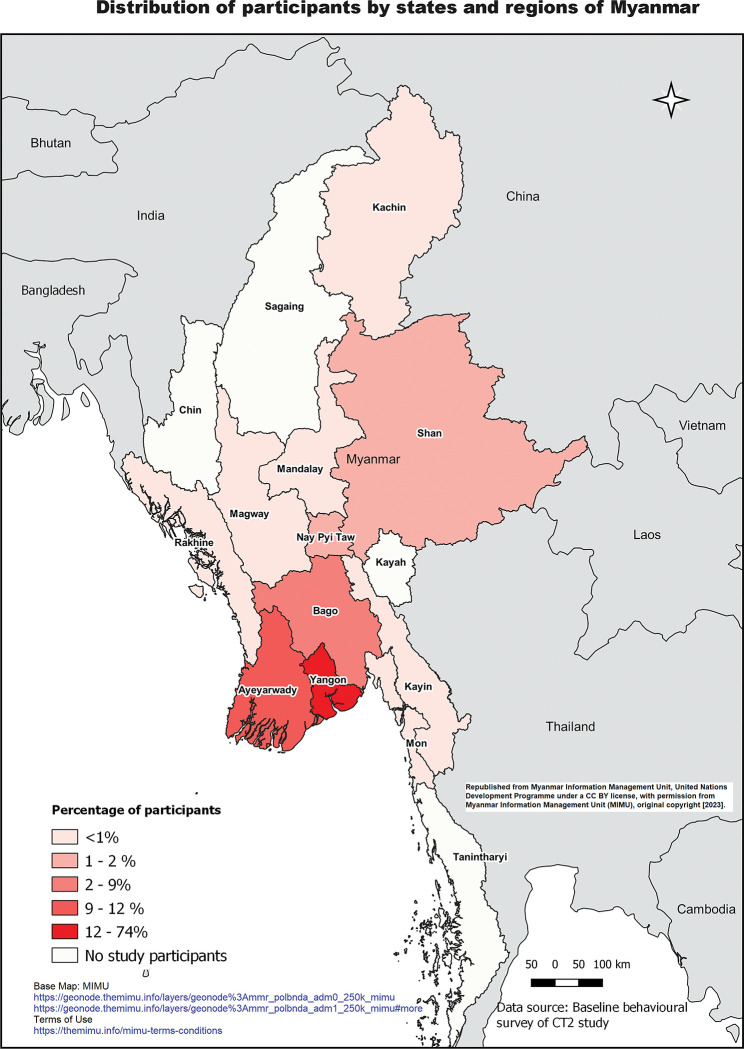
Hepatitis C (HCV) infection elimination in low- and middle-income countries requires decentralised HCV services to increase testing and linkage to care. The CT2 Study investigated patients' views of access to and acceptance of two community-based HCV care models in Myanmar using a mixed-methods approach. Point-of-care HCV testing and general practitioner-initiated HCV treatment were provided at two community clinics in Yangon, Myanmar-the Burnet Institute's (BI) clinic focused on people who inject drugs (PWID), and the Myanmar Liver Foundation's (MLF) clinic focused on people with liver-related diseases. Study staff administered quantitative questionnaires to 633 participants receiving anti-HCV antibody testing. Purposive sampling was used to recruit 29 participants receiving direct-acting antiviral treatment for qualitative interviews. Among participants completing quantitative questionnaires, almost all reported the clinic location was convenient (447/463, 97%), waiting time was acceptable (455/463, 98%), and HCV antibody and RNA testing methods were acceptable (617/632, 98% and 592/605, 97% respectively). Nearly all participants were satisfied with their clinic's services (444/463, 96%) and preferred same-day test results (589/632, 93%). BI clinic participants were more confident that they understood HCV antibody and RNA results; MLF clinic participants were more comfortable disclosing their risk behaviour to staff and had slightly higher satisfaction with the overall care, privacy and secure storage of their information. In qualitative interviews, participants reported that flexible appointment scheduling, short wait times and rapid return of results increased the clinic's accessibility. The simplified point-of-care testing and treatment procedures and supportive healthcare providers contributed to participants' acceptance of the HCV care model. This decentralised community-based HCV testing and treatment model was highly accessible and acceptable to CT2 participants. Prioritizing patient-centred care, rapid provision of results, flexible appointments and convenient clinic locations can promote accessible and acceptable services which may in turn help accelerate progress in reaching HCV elimination targets.
Copyright: © 2023 Yee et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: Margaret Hellard has received investigator-initiated grant funding from Gilead Sciences and Abbvie for unrelated work. Alisa Pedrana has received investigator-initiated grant funding from Gilead Sciences, MSD and Abbvie and speaker fees from Gilead Sciences for unrelated work. Win Lei Yee has received a Gilead Sciences Fellowship for related work. Yi Yi Sein has received non-financial support from Mylan. There is no competing interest for all other authors.
Figures
References
-
- World Health Organization. Global progress report on HIV, viral hepatitis and sexually transmitted infections, 2021. Accountability for the global health sector strategies 2016–2021: actions for impact. Geneva; 2021.
-
- World Health Organization. Hepatitis C: Key Facts: World Health Organization; 2020 [updated 27 July, 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c.
LinkOut - more resources
Full Text Sources