

Gold Nanostars Obviate Limitations to Laser Interstitial Thermal Therapy (LITT) for the Treatment of Intracranial Tumors
- PMID: 37327318
- PMCID: PMC10425731
- DOI: 10.1158/1078-0432.CCR-22-1871
Gold Nanostars Obviate Limitations to Laser Interstitial Thermal Therapy (LITT) for the Treatment of Intracranial Tumors
Abstract
Purpose: Laser interstitial thermal therapy (LITT) is an effective minimally invasive treatment option for intracranial tumors. Our group produced plasmonics-active gold nanostars (GNS) designed to preferentially accumulate within intracranial tumors and amplify the ablative capacity of LITT.
Experimental design: The impact of GNS on LITT coverage capacity was tested in ex vivo models using clinical LITT equipment and agarose gel-based phantoms of control and GNS-infused central "tumors." In vivo accumulation of GNS and amplification of ablation were tested in murine intracranial and extracranial tumor models followed by intravenous GNS injection, PET/CT, two-photon photoluminescence, inductively coupled plasma mass spectrometry (ICP-MS), histopathology, and laser ablation.
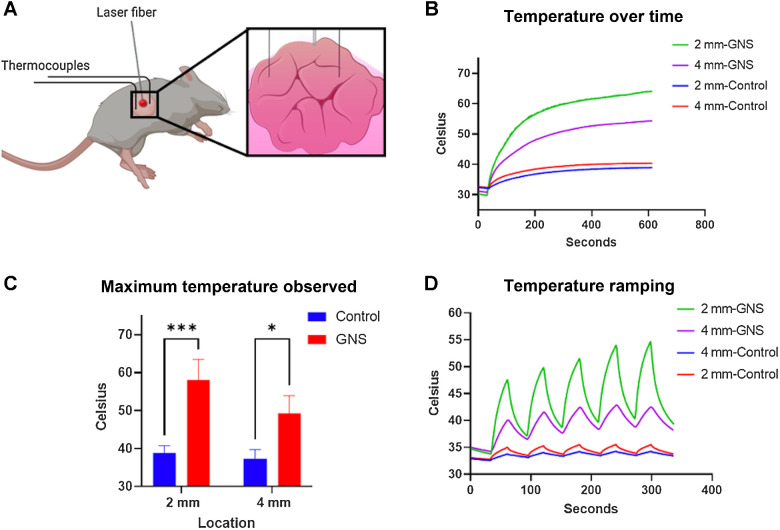
Results: Monte Carlo simulations demonstrated the potential of GNS to accelerate and specify thermal distributions. In ex vivo cuboid tumor phantoms, the GNS-infused phantom heated 5.5× faster than the control. In a split-cylinder tumor phantom, the GNS-infused border heated 2× faster and the surrounding area was exposed to 30% lower temperatures, with margin conformation observed in a model of irregular GNS distribution. In vivo, GNS preferentially accumulated within intracranial tumors on PET/CT, two-photon photoluminescence, and ICP-MS at 24 and 72 hours and significantly expedited and increased the maximal temperature achieved in laser ablation compared with control.
Conclusions: Our results provide evidence for use of GNS to improve the efficiency and potentially safety of LITT. The in vivo data support selective accumulation within intracranial tumors and amplification of laser ablation, and the GNS-infused phantom experiments demonstrate increased rates of heating, heat contouring to tumor borders, and decreased heating of surrounding regions representing normal structures.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures



References
-
- Achrol AS, Rennert RC, Anders C, Soffietti R, Ahluwalia MS, Nayak L, et al. . Brain metastases. Nat Rev Dis Primer 2019;5:1–26. - PubMed
-
- Barnett GH, Voigt JD, Alhuwalia MS. A systematic review and meta-analysis of studies examining the use of brain laser interstitial thermal therapy versus craniotomy for the treatment of high-grade tumors in or near areas of eloquence: an examination of the extent of resection and major complication rates associated with each type of surgery. Ster Funct Neurosurg 2016;94:164–73. - PubMed
-
- Prince E, Hakimian S, Ko AL, Ojemann JG, Kim MS, Miller JW. Laser interstitial thermal therapy for epilepsy. Curr Neurol Neurosci Rep 2017;17:63. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
