

CD36 Drives Metastasis and Relapse in Acute Myeloid Leukemia
- PMID: 37327406
- PMCID: PMC10472106
- DOI: 10.1158/0008-5472.CAN-22-3682
CD36 Drives Metastasis and Relapse in Acute Myeloid Leukemia
Abstract
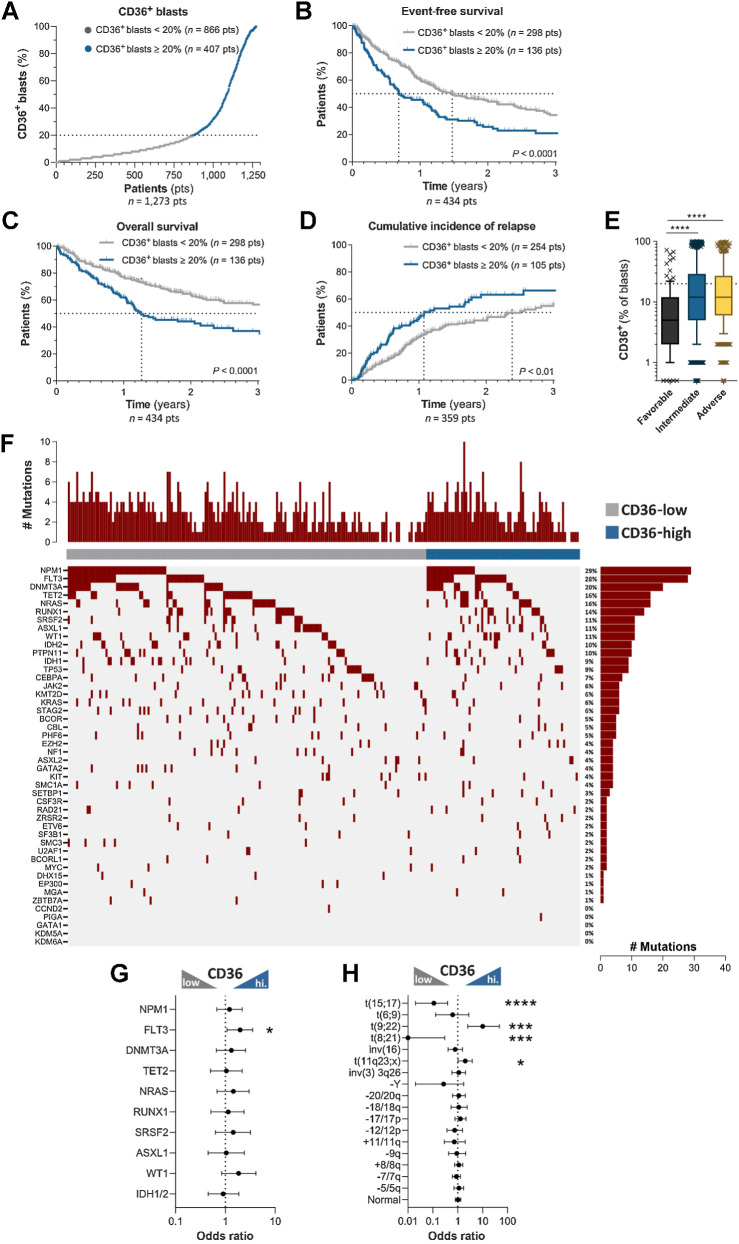
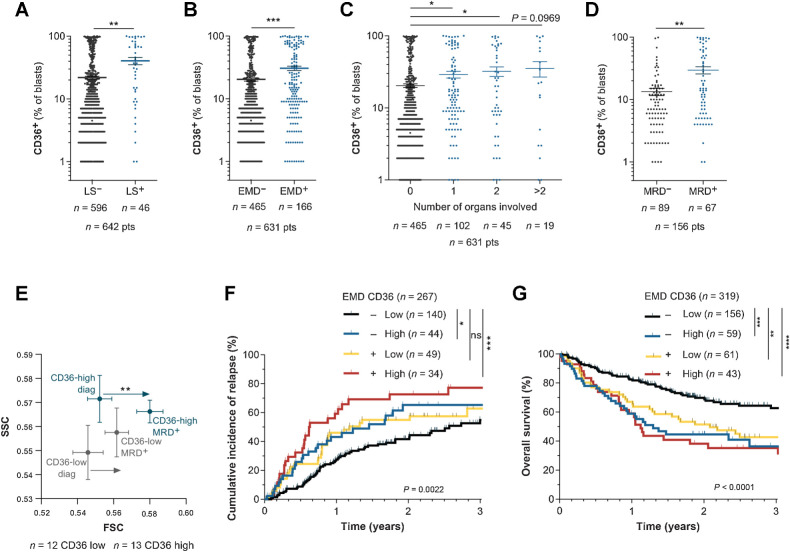
Identifying mechanisms underlying relapse is a major clinical issue for effective cancer treatment. The emerging understanding of the importance of metastasis in hematologic malignancies suggests that it could also play a role in drug resistance and relapse in acute myeloid leukemia (AML). In a cohort of 1,273 AML patients, we uncovered that the multifunctional scavenger receptor CD36 was positively associated with extramedullary dissemination of leukemic blasts, increased risk of relapse after intensive chemotherapy, and reduced event-free and overall survival. CD36 was dispensable for lipid uptake but fostered blast migration through its binding with thrombospondin-1. CD36-expressing blasts, which were largely enriched after chemotherapy, exhibited a senescent-like phenotype while maintaining their migratory ability. In xenograft mouse models, CD36 inhibition reduced metastasis of blasts and prolonged survival of chemotherapy-treated mice. These results pave the way for the development of CD36 as an independent marker of poor prognosis in AML patients and a promising actionable target to improve the outcome of patients.
Significance: CD36 promotes blast migration and extramedullary disease in acute myeloid leukemia and represents a critical target that can be exploited for clinical prognosis and patient treatment.
©2023 The Authors; Published by the American Association for Cancer Research.
Figures
![Figure 2. CD36 inhibition delays AML relapse after chemotherapy. A, Percentage of mice engrafted with U937 cells transduced with shCtrl (n = 11) or shCD36 (n = 11) and treated with vehicle or AraC, surviving over time after treatment. B, Same as A, with OCIAML3 [shCtrl (n = 18) and shCD36 (n = 22)]. C, Percentage of mice engrafted with U937 cells surviving over time after treatment with the indicated combinations of PBS or AraC administered for the first 5 days, with either control IgG or FA6-152 anti-CD36 antibody injected three times/week (n = 7 PBS-IGG; n = 7 PBS-anti-CD36; n = 7 AraC-IGG; n = 6 AraC-anti-CD36). D, Venn diagram of significantly cooverexpressed genes along with CD36 in TCGA, Verhaak, and BeatAML cohorts. E, Gene set enrichment analysis of CD36 gene signature in AraC versus untreated AML blasts from three different transcriptomic analyses. A–C, log-rank (Mantel–Cox) test. E, One sample t test. *, P < 0.05; **, P < 0.01; ***, P < 0.001; ****, P < 0.0001; ns, not significant.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/045d/10472106/e4459769aa47/2824fig2.jpg)
![Figure 3. CD36 triggers blast migration. A, GO analysis of migration-related biological processes significantly enriched in the CD36 gene signature. B, Number of migrating shCtrl or shCD36 U937 cells in the lower chamber of the transwell assay (normalized to control; n = 5). C, As in B, but with CD36-blocking antibodies (FA6-152 or JC53.1; n = 4). D, Number of migrating cells in primary AML samples treated or not with CD36 blocking antibody (FA6-152; n = 7). E, Number of migrating shCtrl or shTSP1 U937 cells (normalized to control; n = 3). F, Number of migrating shCtrl or shCD36 U937 cells treated or not with TSP1-blocking antibody (A6.1; normalized to shCtrl; n = 5). G, Number of migrating U937 cells treated or not with recombinant TSP1 in the presence or not of CD36-blocking antibody (FA6-152; normalized to control; n = 3). H, As in D, but with TSP1-blocking antibody (A6.1; n = 5). I, Bioluminescence imaging of mice injected with the indicated AML cell line stably expressing a luciferase reporter from day 1 to day 64 after injection. J, Representative histologic section showing anti-human Ku-80 labeling of U937 AML blasts in the subcutaneous adipose tissue 17 days after xenograft. Positive brown nuclei highlight the infiltration of human blasts in murine adipose tissue either as dense infiltrate (top) or scattered isolated cells (bottom). Top scale bar, 50 μm; bottom, 10 μm. K, Percentage of viable OCIAML3 cells in the indicated tissues 14 days after orthotopic injection in the femur. L, Expression of CD36 [mean fluorescence intensity (MFI)] in viable OCIAML3 cells measured in the injected and contralateral femur and different organs of mice 14 days after orthotopic injection. Values are represented as mean ± SEM. B, C, and E, One sample t test. D and H, Paired t test. F and G, Ordinary one-way ANOVA with Tukey multiple comparisons test. L, Matched one-way ANOVA. *, P < 0.05; **, P < 0.01; ***, P < 0.001; ****, P < 0.0001; ns, not significant.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/045d/10472106/94de82caa0e3/2824fig3.jpg)
References
-
- Short NJ, Konopleva M, Kadia TM, Borthakur G, Ravandi F, DiNardo CD, et al. . Advances in the treatment of acute myeloid leukemia: new drugs and new challenges. Cancer Discov 2020;10:506–25. - PubMed
-
- Boyd AL, Aslostovar L, Reid J, Ye W, Tanasijevic B, Porras DP, et al. . Identification of chemotherapy-induced leukemic-regenerating cells reveals a transient vulnerability of human AML recurrence. Cancer Cell 2018;34:483–98. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
