

Medicaid expansion and risk of eclampsia
- PMID: 37330007
- PMCID: PMC10527027
- DOI: 10.1016/j.ajogmf.2023.101054
Medicaid expansion and risk of eclampsia
Abstract
Background: Eclampsia is an indicator of severe maternal morbidity and can be prevented through increased prenatal care access and early prenatal care utilization. The 2014 Medicaid expansion under the Patient Protection and Affordable Care Act allowed states to expand Medicaid coverage to nonelderly adults with incomes up to 138% of the federal poverty level. Its implementation has led to a significant increase in prenatal care access and utilization.
Objective: This study aimed to assess the association of Medicaid expansion under the Affordable Care Act with eclampsia incidence.
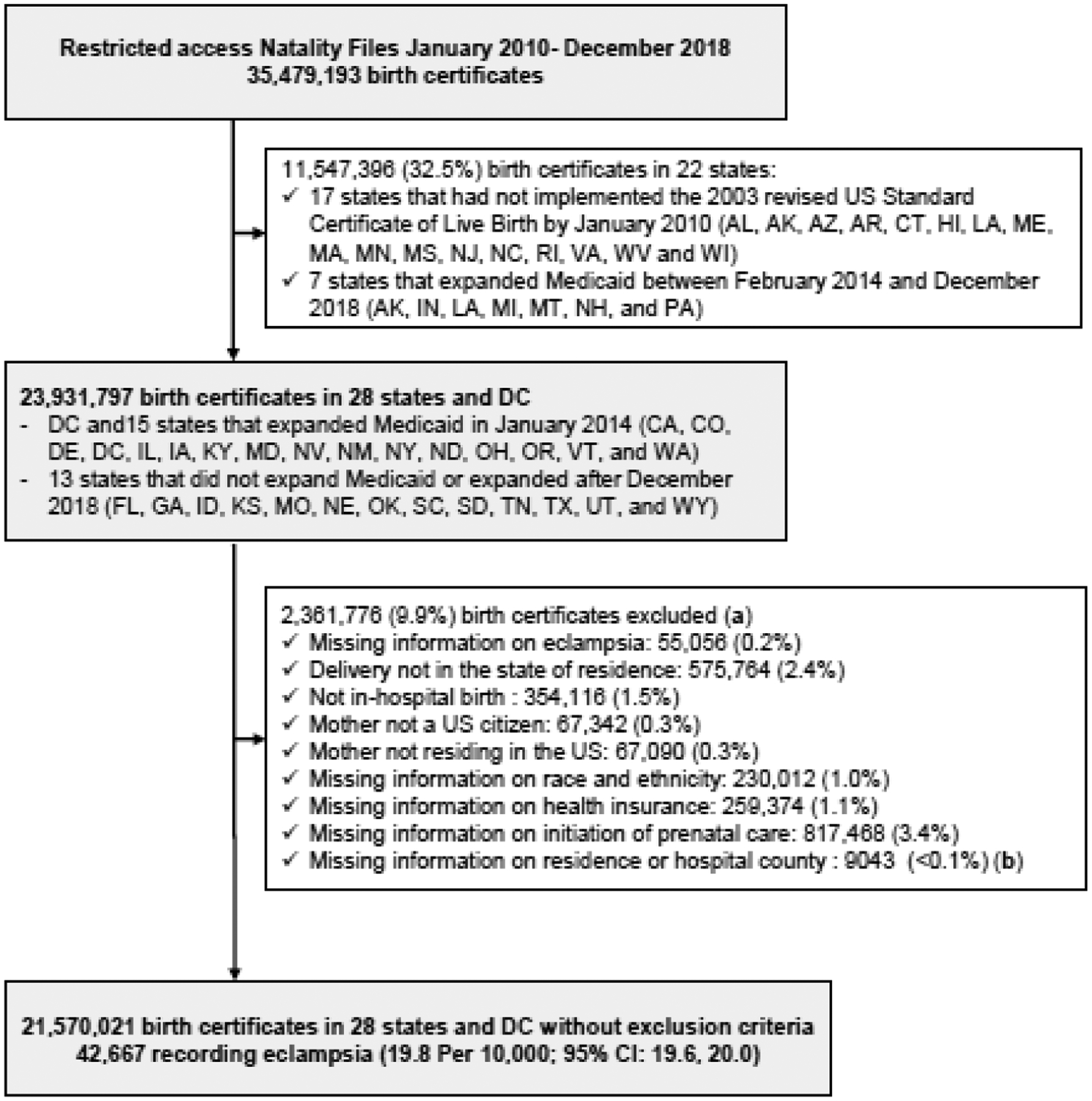
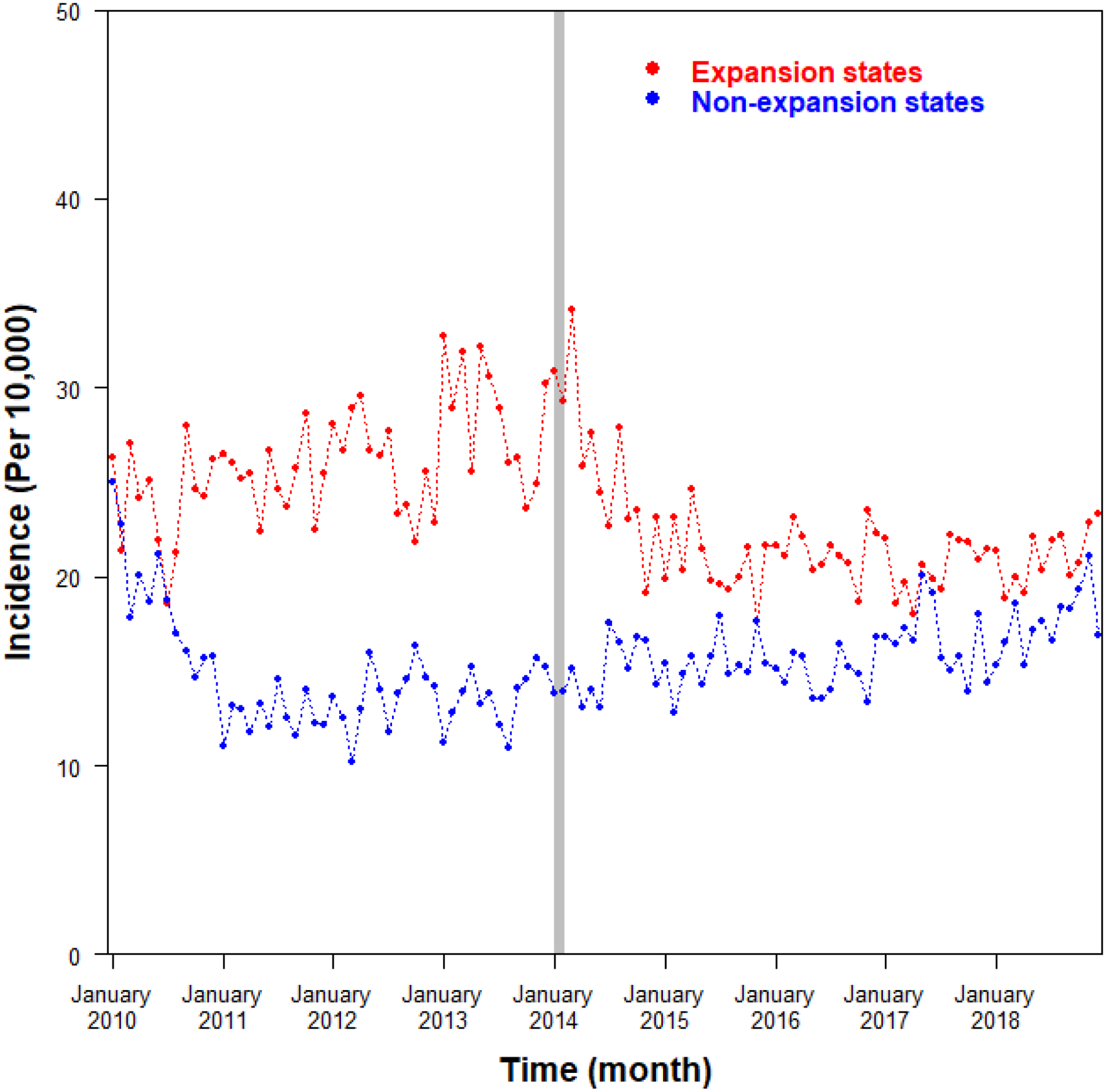
Study design: This natural experiment study was based on US birth certificate data from January 2010 to December 2018 in 16 states that expanded Medicaid in January 2014 and in 13 states that did not expand Medicaid during the study period. The outcome was eclampsia incidence, the intervention was the implementation of the Medicaid expansion, and the exposure was state expansion status. Using the interrupted time series method, we compared temporal trends in the incidence of eclampsia before and after the intervention in expansion vs non-expansion states with adjustments for patient and hospital county characteristics.
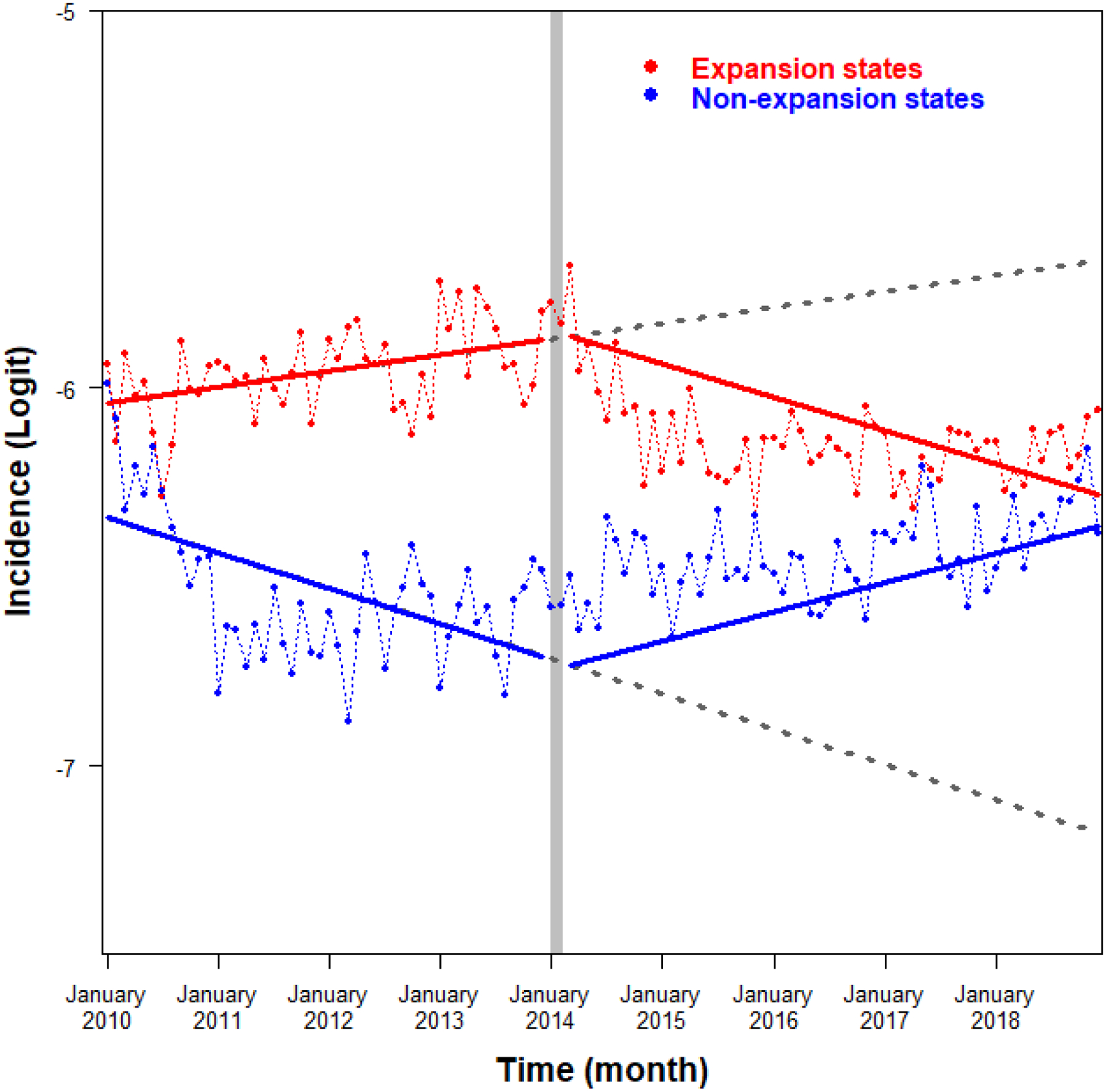
Results: Of the 21,570,021 birth certificates analyzed, 11,433,862 (53.0%) were in expansion states and 12,035,159 (55.8%) were in the postintervention period. The diagnosis of eclampsia was recorded in 42,677 birth certificates or 19.8 per 10,000 (95% confidence interval, 19.6-20.0). The incidence of eclampsia was higher for Black people (29.1 per 10,000) than for White (20.7 per 10,000), Hispanic (15.3 per 10,000), and birthing people of other race and ethnicity (15.4 per 10,000). In the expansion states, the incidence of eclampsia increased during the preintervention period and decreased during the postintervention period; in the nonexpansion states, a reverse pattern was observed. A statistically significant difference was observed between expansion and nonexpansion states in temporal trends between the pre- and postintervention periods, with an overall 1.6% decrease (95% confidence interval, 1.3-1.9) in the incidence of eclampsia in expansion states compared with nonexpansion states. The results were consistent in subgroup analyses according to maternal race and ethnicity, education level (less than high school or high school and higher), parity (nulliparous or parous), delivery mode (vaginal or cesarean delivery), and poverty in the residence county (high or low).
Conclusion: Implementation of the Affordable Care Act Medicaid expansion was associated with a small statistically significant reduction in the incidence of eclampsia. Its clinical significance and cost-effectiveness remain to be determined.
Keywords: Medicaid expansion; childbirth; eclampsia; epidemiology; health policy; hypertensive disorders of pregnancy; maternal mortality; severe maternal morbidity.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
COMPETING INTERESTS
The authors report no conflict of interest.
Figures
Similar articles
-
Impact of Medicaid expansion on women with gynecologic cancer: a difference-in-difference analysis.Am J Obstet Gynecol. 2021 Feb;224(2):195.e1-195.e17. doi: 10.1016/j.ajog.2020.08.007. Epub 2020 Aug 7. Am J Obstet Gynecol. 2021. PMID: 32777264 Free PMC article.
-
Analysis of State Medicaid Expansion and Access to Timely Prenatal Care Among Women Who Were Immigrant vs US Born.JAMA Netw Open. 2022 Oct 3;5(10):e2239264. doi: 10.1001/jamanetworkopen.2022.39264. JAMA Netw Open. 2022. PMID: 36306127 Free PMC article.
-
Preconception Coverage Before and After the Affordable Care Act Medicaid Expansions.Obstet Gynecol. 2018 Dec;132(6):1394-1400. doi: 10.1097/AOG.0000000000002972. Obstet Gynecol. 2018. PMID: 30399105
-
Association of Medicaid Expansion With Coverage and Access to Care for Pregnant Women.Obstet Gynecol. 2019 Nov;134(5):1066-1074. doi: 10.1097/AOG.0000000000003501. Obstet Gynecol. 2019. PMID: 31599841
-
Comparison of Insurance Status and Diagnosis Stage Among Patients With Newly Diagnosed Cancer Before vs After Implementation of the Patient Protection and Affordable Care Act.JAMA Oncol. 2018 Dec 1;4(12):1713-1720. doi: 10.1001/jamaoncol.2018.3467. JAMA Oncol. 2018. PMID: 30422152 Free PMC article.
Cited by
-
State-Level Indicators of Structural Racism and Severe Adverse Maternal Outcomes During Childbirth.Matern Child Health J. 2024 Jan;28(1):165-176. doi: 10.1007/s10995-023-03828-9. Epub 2023 Nov 8. Matern Child Health J. 2024. PMID: 37938439 Free PMC article.
-
Reduced odds of severe maternal morbidity associated with the US Affordable Care Act dependent coverage provision.Am J Obstet Gynecol MFM. 2025 Jun;7(6):101668. doi: 10.1016/j.ajogmf.2025.101668. Epub 2025 Mar 11. Am J Obstet Gynecol MFM. 2025. PMID: 40081762
References
-
- Fishel Bartal M, Sibai BM. Eclampsia in the 21st century. Am J Obstet Gynecol 2022;226:S1237–S53. - PubMed
-
- American College of Obstetricians and Gynecologists. Gestational hypertension and preeclampsia: ACOG Practice Bulletin, number 222. Obstet Gynecol 2020;135:e237–e60. - PubMed
-
- Xiao MZX, Whitney D, Guo N, et al. Trends in eclampsia in the United States, 2009–2017: a population-based study. J Hypertens 2022;40:490–97. - PubMed
-
- Fingar KR, Mabry-Hernandez I, Ngo-Metzger Q, Wolff T, Steiner CA, Elixhauser A. Delivery hospitalizations involving preeclampsia and eclampsia, 2005–2014. Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD), 2006. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
