

Third International Consensus Conference on lesions of uncertain malignant potential in the breast (B3 lesions)
- PMID: 37330436
- PMCID: PMC10326140
- DOI: 10.1007/s00428-023-03566-x
Third International Consensus Conference on lesions of uncertain malignant potential in the breast (B3 lesions)
Abstract
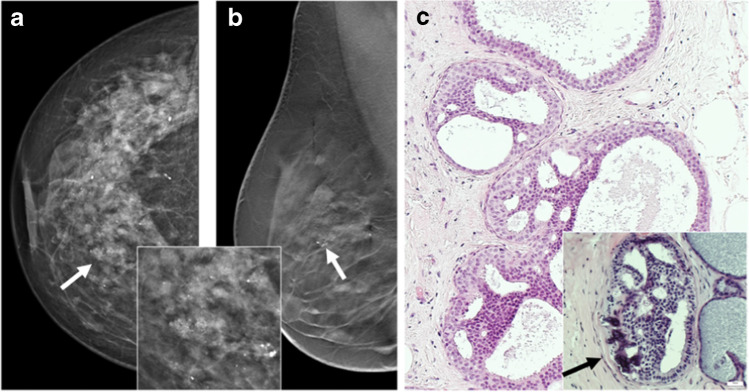
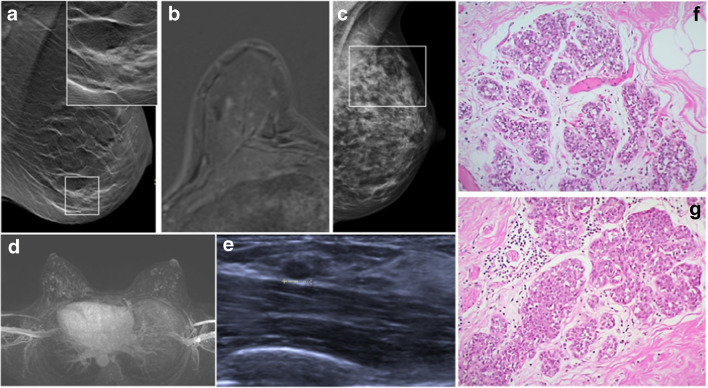
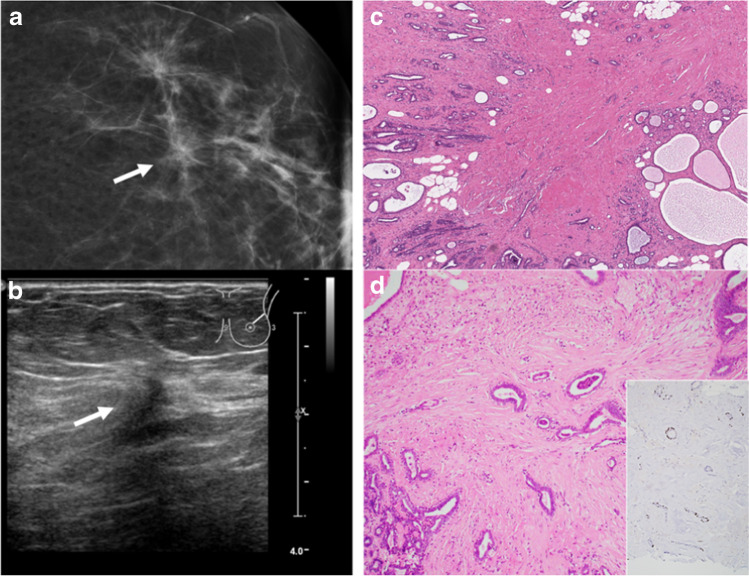
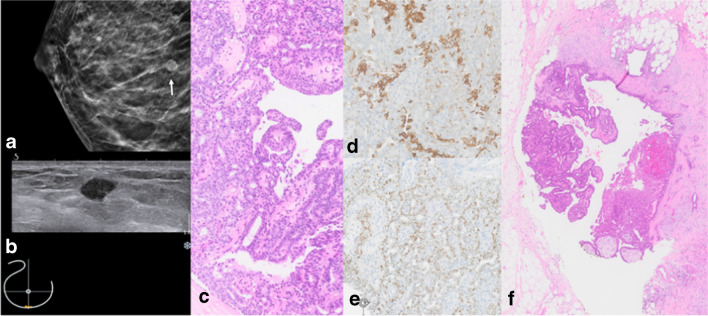
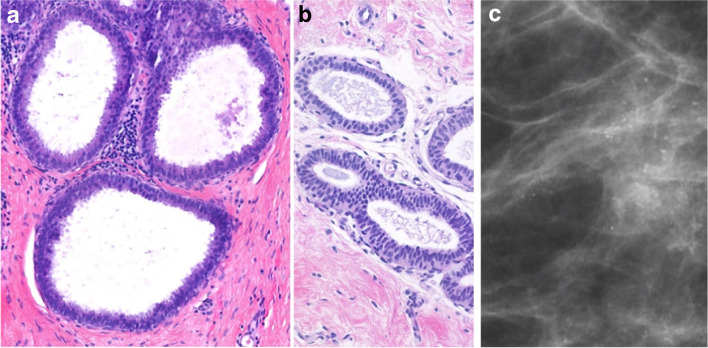
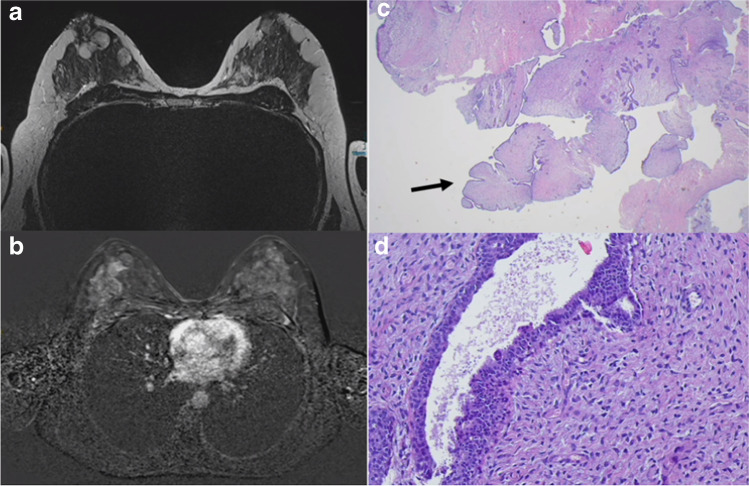
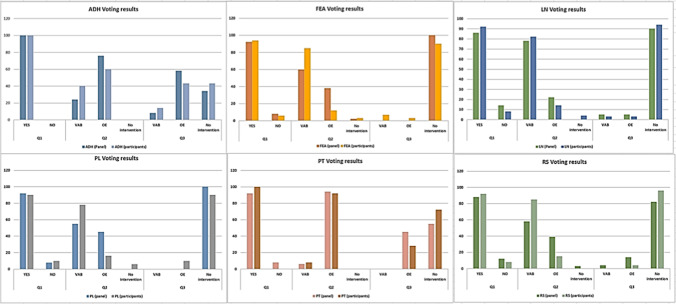
The heterogeneous group of B3 lesions in the breast harbors lesions with different malignant potential and progression risk. As several studies about B3 lesions have been published since the last Consensus in 2018, the 3rd International Consensus Conference discussed the six most relevant B3 lesions (atypical ductal hyperplasia (ADH), flat epithelial atypia (FEA), classical lobular neoplasia (LN), radial scar (RS), papillary lesions (PL) without atypia, and phyllodes tumors (PT)) and made recommendations for diagnostic and therapeutic approaches. Following a presentation of current data of each B3 lesion, the international and interdisciplinary panel of 33 specialists and key opinion leaders voted on the recommendations for further management after core-needle biopsy (CNB) and vacuum-assisted biopsy (VAB). In case of B3 lesion diagnosis on CNB, OE was recommended in ADH and PT, whereas in the other B3 lesions, vacuum-assisted excision was considered an equivalent alternative to OE. In ADH, most panelists (76%) recommended an open excision (OE) after diagnosis on VAB, whereas observation after a complete VAB-removal on imaging was accepted by 34%. In LN, the majority of the panel (90%) preferred observation following complete VAB-removal. Results were similar in RS (82%), PL (100%), and FEA (100%). In benign PT, a slim majority (55%) also recommended an observation after a complete VAB-removal. VAB with subsequent active surveillance can replace an open surgical intervention for most B3 lesions (RS, FEA, PL, PT, and LN). Compared to previous recommendations, there is an increasing trend to a de-escalating strategy in classical LN. Due to the higher risk of upgrade into malignancy, OE remains the preferred approach after the diagnosis of ADH.
Keywords: ADH; B3 lesion; Breast surgery; Consensus; Core-needle biopsy; FEA; LN; Papilloma; Phyllodes tumor; Radial Scar; Uncertain malignant potential; Vacuum-assisted biopsy; Vacuum-assisted excision.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- AGO German Commission Breast SoAG. AGO German Commission Breast, State of Art Guidelines 2022 2022 [Available from: https://www.ago-online.de/en/leitlinien-empfehlungen/leitlinien-empfehlu.... Accessed 15 Jan 2023
-
- S3-Richtlinien. Deutsche Krebsgesellschaft, Deutsche Krebshilfe, AWMF. S3-Leitlinie Früherkennung, Diagnose, Therapie und Nachsorge des Mammakarzinoms, Version 4.4. Mai 2021 2021 [Available from: https://www.awmf.org/uploads/tx_szleitlinien/032-045OLl_S3_Mammakarzinom.... Accessed 15 Jan 2023
-
- WHO. Breast Tumours WHO Classification of Tumours, 5th Edition2019. https://nottingham-repository.worktribe.com/output/4758580. Accessed 15 Jan 2023
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
