

Prone position versus usual care in hypoxemic COVID-19 patients in medical wards: a randomised controlled trial
- PMID: 37330512
- PMCID: PMC10276908
- DOI: 10.1186/s13054-023-04529-z
Prone position versus usual care in hypoxemic COVID-19 patients in medical wards: a randomised controlled trial
Abstract
Background: Benefit of early awake prone positioning for COVID-19 patients hospitalised in medical wards and who need oxygen therapy remains to be demonstrated. The question was considered at the time of COVID-19 pandemic to avoid overloading the intensive care units. We aimed to determine whether prone position plus usual care could reduce the rate of non-invasive ventilation (NIV) or intubation or death as compared to usual care alone.
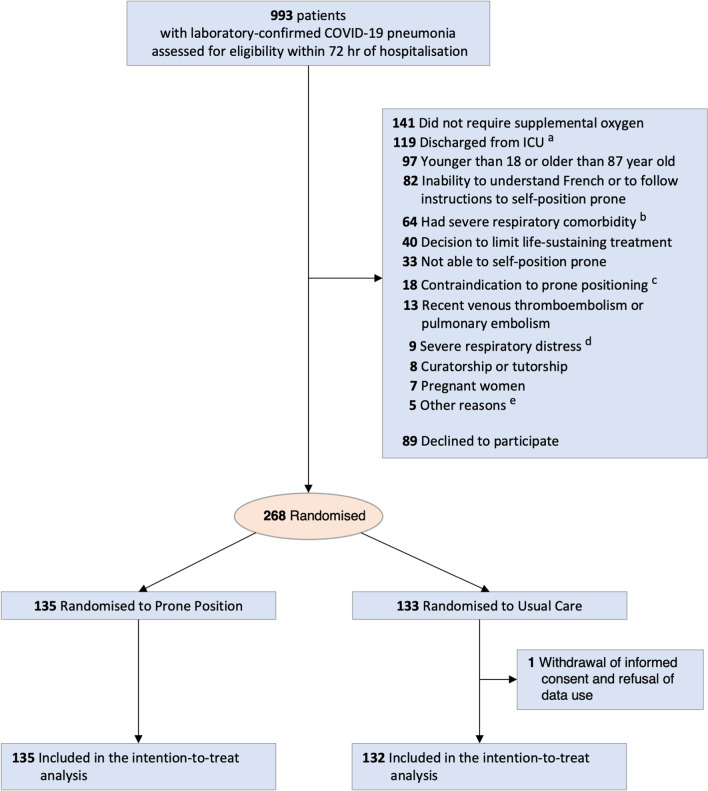
Methods: In this multicentre randomised clinical trial, 268 patients were randomly assigned to awake prone position plus usual care (N = 135) or usual care alone (N = 132). The primary outcome was the proportion of patients who underwent NIV or intubation or died within 28 days. Main secondary outcomes included the rates of NIV, of intubation or death, within 28 days.
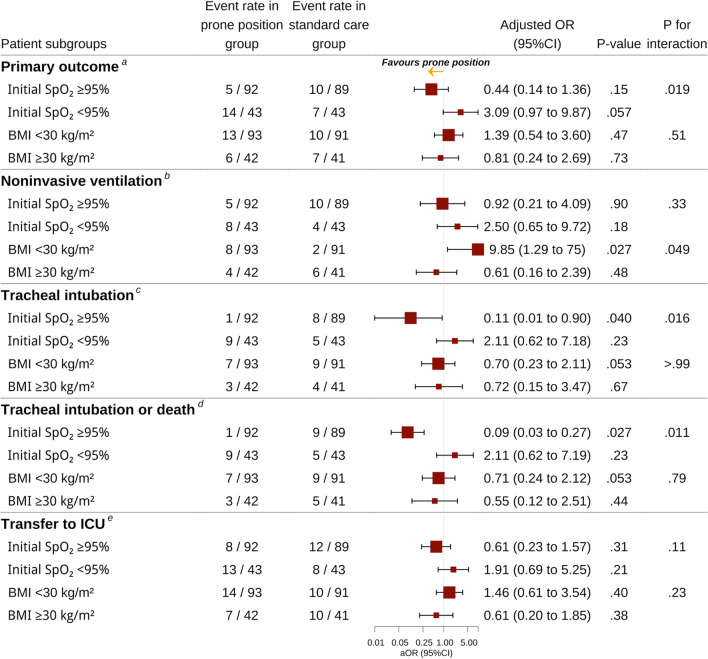
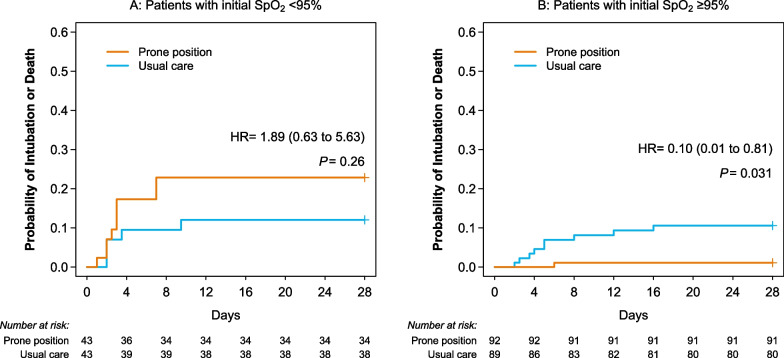
Results: Median time spent each day in the prone position within 72 h of randomisation was 90 min (IQR 30-133). The proportion of NIV or intubation or death within 28 days was 14.1% (19/135) in the prone position group and 12.9% (17/132) in the usual care group [odds ratio adjusted for stratification (aOR) 0.43; 95% confidence interval (CI) 0.14-1.35]. The probability of intubation, or intubation or death (secondary outcomes) was lower in the prone position group than in the usual care group (aOR 0.11; 95% CI 0.01-0.89 and aOR 0.09; 95% CI 0.01-0.76, respectively) in the whole study population and in the prespecified subgroup of patients with SpO2 ≥ 95% on inclusion (aOR 0.11; 95% CI 0.01-0.90, and aOR 0.09; 95% CI 0.03-0.27, respectively).
Conclusions: Awake prone position plus usual care in COVID-19 patients in medical wards did not decrease the composite outcome of need for NIV or intubation or death. Trial registration ClinicalTrials.gov Identifier: NCT04363463 . Registered 27 April 2020.
Keywords: Awake prone position; COVID-19; Hypoxemia; Medical wards; Non-intubated; Respiratory failure; Spontaneous breathing.
© 2023. The Author(s).
Conflict of interest statement
There are no competing interests for any author concerning the submitted work. MAN has received financial research support, materials supports and personal fees from Fisher&Paykel Healthcare outside the submitted work and congress and travel reimbursement from Pfizer.
There are no competing interests for any author concerning the submitted work. MAN has received financial research support, materials supports and personal fees from Fisher & Paykel Healthcare outside the submitted work and congress and travel reimbursement from Pfizer.
Figures
Comment in
-
Lung physiological changes during awake prone positioning in non-intubated hypoxemia patients.Crit Care. 2023 Oct 13;27(1):393. doi: 10.1186/s13054-023-04672-7. Crit Care. 2023. PMID: 37833716 Free PMC article. No abstract available.
-
Prone position versus usual care in hypoxemic COVID-19 patients in medical wards: a randomised controlled trial.J Thorac Dis. 2023 Nov 30;15(11):6379-6381. doi: 10.21037/jtd-23-1342. Epub 2023 Nov 17. J Thorac Dis. 2023. PMID: 38090329 Free PMC article. No abstract available.
-
When hope meets reality: the challenges of awake proning in unmonitored settings.J Thorac Dis. 2024 Jan 30;16(1):810-815. doi: 10.21037/jtd-23-1588. Epub 2023 Dec 11. J Thorac Dis. 2024. PMID: 38410573 Free PMC article. No abstract available.
-
Awake prone positioning in COVID-19 patients: is there any benefit?J Thorac Dis. 2024 Jan 30;16(1):807-809. doi: 10.21037/jtd-23-1389. Epub 2024 Jan 11. J Thorac Dis. 2024. PMID: 38410584 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
