

Increased red blood cell deformation in children and adolescents after SARS-CoV-2 infection
- PMID: 37330522
- PMCID: PMC10276822
- DOI: 10.1038/s41598-023-35692-6
Increased red blood cell deformation in children and adolescents after SARS-CoV-2 infection
Abstract
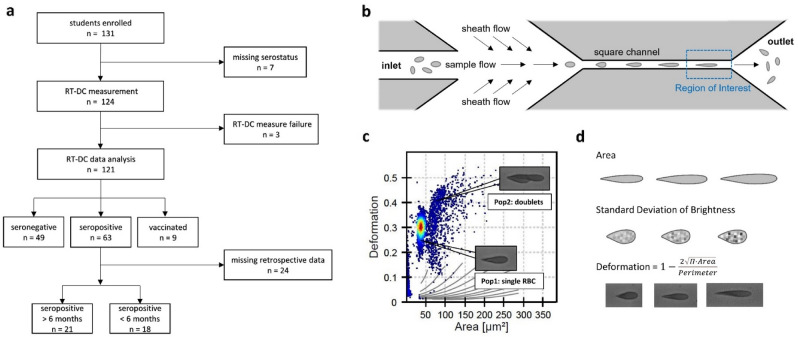
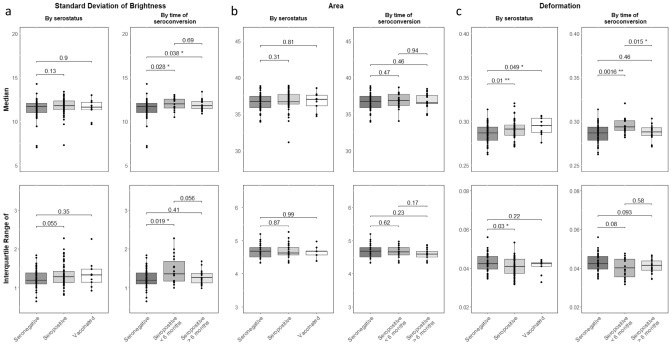
Severe coronavirus disease 2019 (COVID-19) is associated with hyperinflammation, hypercoagulability and hypoxia. Red blood cells (RBCs) play a key role in microcirculation and hypoxemia and are therefore of special interest in COVID-19 pathophysiology. While this novel disease has claimed the lives of many older patients, it often goes unnoticed or with mild symptoms in children. This study aimed to investigate morphological and mechanical characteristics of RBCs after SARS-CoV-2 infection in children and adolescents by real-time deformability-cytometry (RT-DC), to investigate the relationship between alterations of RBCs and clinical course of COVID-19. Full blood of 121 students from secondary schools in Saxony, Germany, was analyzed. SARS-CoV-2-serostatus was acquired at the same time. Median RBC deformation was significantly increased in SARS-CoV-2-seropositive compared to seronegative children and adolescents, but no difference could be detected when the infection dated back more than 6 months. Median RBC area was the same in seropositive and seronegative adolescents. Our findings of increased median RBC deformation in SARS-CoV-2 seropositive children and adolescents until 6 months post COVID-19 could potentially serve as a progression parameter in the clinical course of the disease with an increased RBC deformation pointing towards a mild course of COVID-19.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
