

Long-term effects of restriction of intravenous fluid in adult ICU patients with septic shock
- PMID: 37330928
- PMCID: PMC10354110
- DOI: 10.1007/s00134-023-07114-8
Long-term effects of restriction of intravenous fluid in adult ICU patients with septic shock
Abstract
Purpose: To assess long-term outcomes of restrictive versus standard intravenous (IV) fluid therapy in adult intensive care unit (ICU) patients with septic shock included in the European Conservative versus Liberal Approach to Fluid Therapy in Septic Shock in Intensive Care (CLASSIC) trial.
Methods: We conducted the pre-planned analyses of mortality, health-related quality of life (HRQoL) using EuroQol (EQ)-5D-5L index values and EQ visual analogue scale (VAS), and cognitive function using Mini Montreal Cognitive Assessment (Mini MoCA) test at 1 year. Deceased patients were assigned numerical zero for HRQoL as a state equal to death and zero for cognitive function outcomes as worst possible score, and we used multiple imputation for missing data on HRQoL and cognitive function.
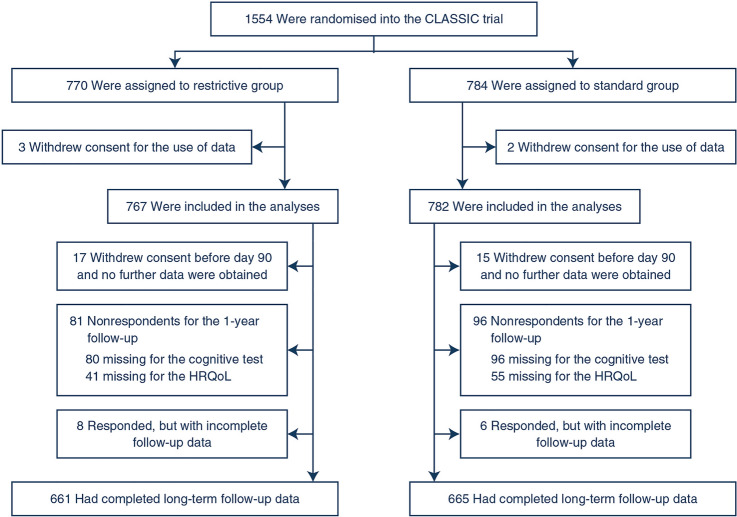
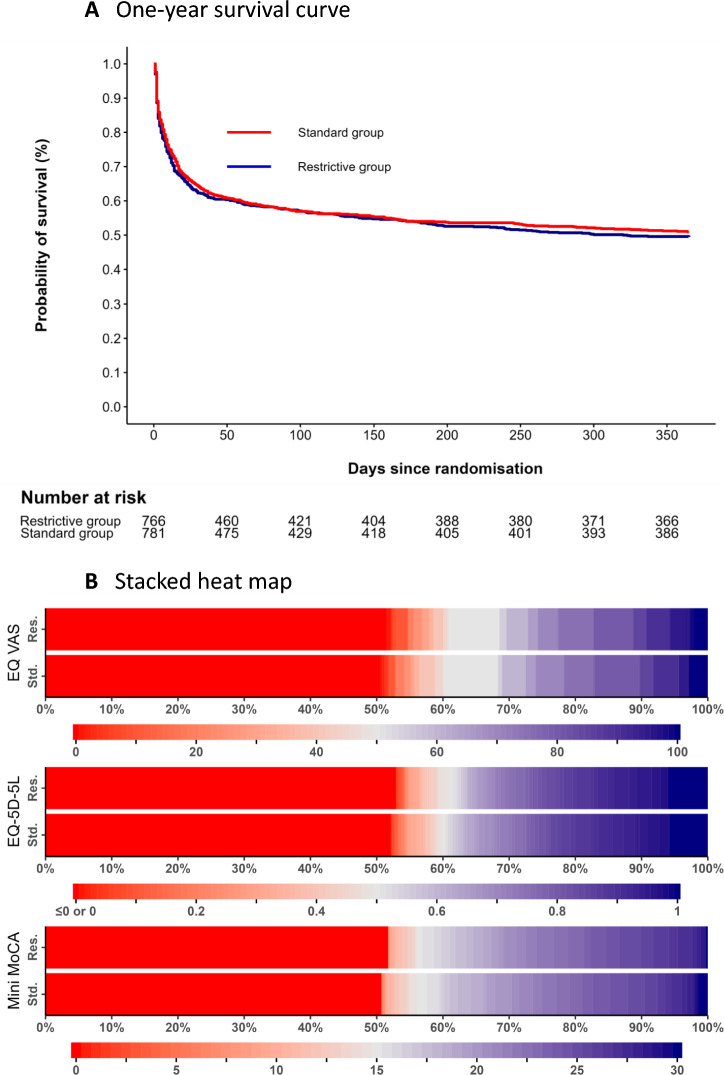
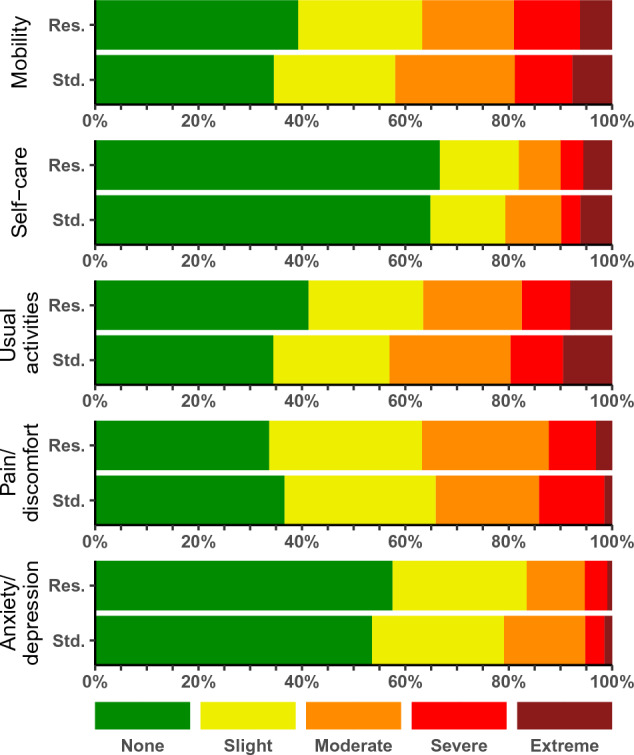
Results: Among 1554 randomized patients, we obtained 1-year data on mortality in 97.9% of patients, HRQoL in 91.3%, and cognitive function in 86.3%. One-year mortality was 385/746 (51.3%) in the restrictive-fluid group versus 383/767 (49.9%) in the standard-fluid group, absolute risk difference 1.5%-points [99% confidence interval (CI) - 4.8 to 7.8]. Mean differences were 0.00 (99% CI - 0.06 to 0.05) for EQ-5D-5L index values, - 0.65 for EQ VAS (- 5.40 to 4.08), and - 0.14 for Mini MoCA (- 1.59 to 1.14) for the restrictive-fluid group versus the standard-fluid group. The results for survivors only were similar in both groups.
Conclusions: Among adult ICU patients with septic shock, restrictive versus standard IV fluid therapy resulted in similar survival, HRQoL, and cognitive function at 1 year, but clinically important differences could not be ruled out.
Trial registration: ClinicalTrials.gov NCT03668236.
Keywords: Cognitive function; Critical illness; Intravenous fluid; Long-term outcomes; Quality of life; Sepsis; Septic shock.
© 2023. The Author(s).
Conflict of interest statement
MBNK, TSM, PS, AG, PBH, MBM, MHM, GVK, and AP are affiliated with the Department of Intensive Care at Rigshospitalet, which has received funding for other projects from The Novo Nordisk Foundation, Pfizer, and Fresenius Kabi, Sygeforsikringen “danmark”, and has conducted contract research for AM-Pharma (the REVIVAL trial). AP has received an honorarium from Novartis for the participation in an advisory board. MHB and SW are affiliated with the Department of Anaesthesia and Intensive Care at Copenhagen University Hospital – North Zealand, which has received funding for other research projects from The Novo Nordisk Foundation, Sygeforsikringen “danmark”, Toyota Foundation, A.P. Moeller Foundation, Frimodt-Heineke Foundation, Svend Andersen Foundation, Ehrenreich Foundation, and Olga Bryde Nielsen Foundation, and has conducted contract research for AM-Pharma (the REVIVAL trial) and Inotrem (ASTONISH trial). MHB has received an honorarium from AM-Pharma for participation in an advisory board. All other authors have no conflicts to disclose.
Figures
Comment on
-
Long-term patient-important outcomes after septic shock: A protocol for 1-year follow-up of the CLASSIC trial.Acta Anaesthesiol Scand. 2020 Mar;64(3):410-416. doi: 10.1111/aas.13519. Epub 2019 Dec 26. Acta Anaesthesiol Scand. 2020. PMID: 31828753
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
