

Effectiveness of Lumbar Cerebrospinal Fluid Drain Among Patients With Aneurysmal Subarachnoid Hemorrhage: A Randomized Clinical Trial
- PMID: 37330974
- PMCID: PMC10277935
- DOI: 10.1001/jamaneurol.2023.1792
Effectiveness of Lumbar Cerebrospinal Fluid Drain Among Patients With Aneurysmal Subarachnoid Hemorrhage: A Randomized Clinical Trial
Erratum in
-
Error in Figure 2.JAMA Neurol. 2023 Aug 1;80(8):873. doi: 10.1001/jamaneurol.2023.3002. JAMA Neurol. 2023. PMID: 37578477 Free PMC article. No abstract available.
Abstract
Importance: After aneurysmal subarachnoid hemorrhage, the use of lumbar drains has been suggested to decrease the incidence of delayed cerebral ischemia and improve long-term outcome.
Objective: To determine the effectiveness of early lumbar cerebrospinal fluid drainage added to standard of care in patients after aneurysmal subarachnoid hemorrhage.
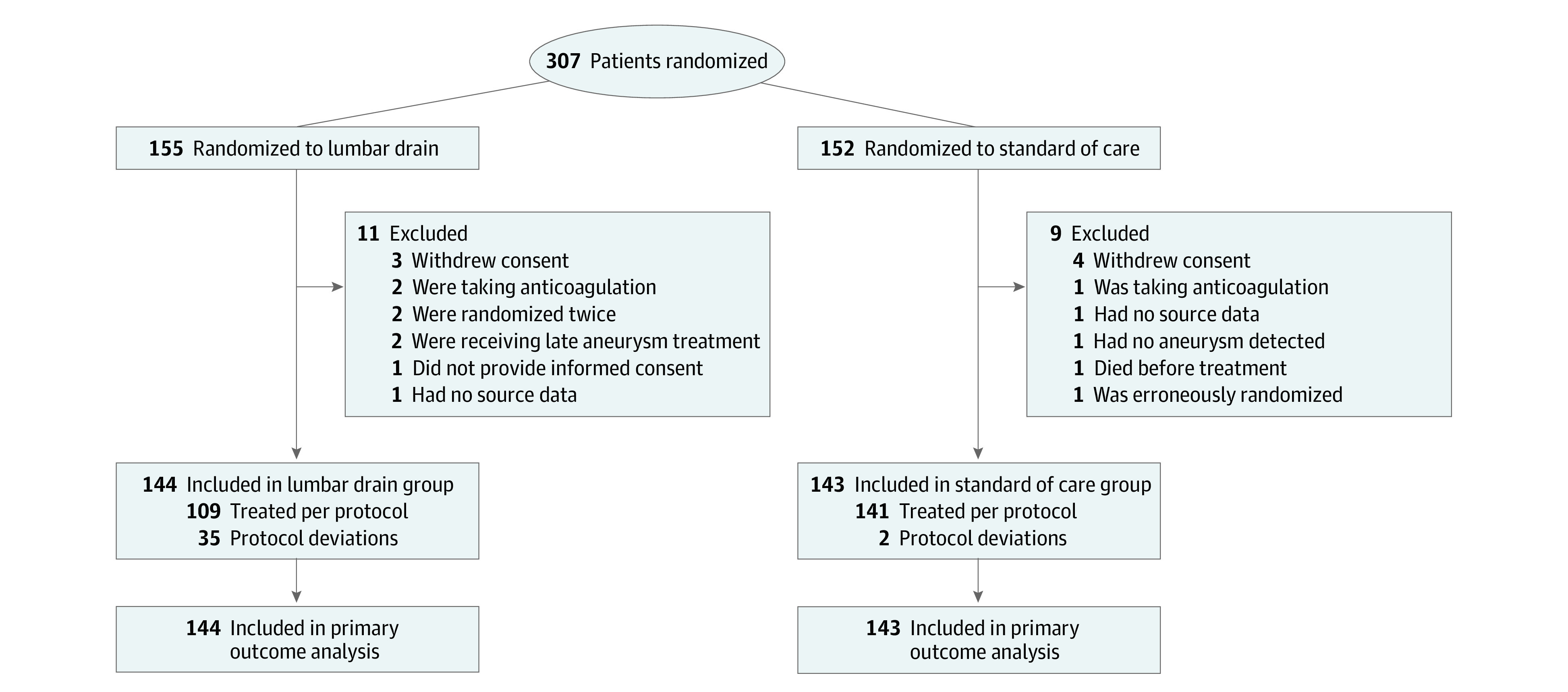
Design, setting, and participants: The EARLYDRAIN trial was a pragmatic, multicenter, parallel-group, open-label randomized clinical trial with blinded end point evaluation conducted at 19 centers in Germany, Switzerland, and Canada. The first patient entered January 31, 2011, and the last on January 24, 2016, after 307 randomizations. Follow-up was completed July 2016. Query and retrieval of data on missing items in the case report forms was completed in September 2020. A total of 20 randomizations were invalid, the main reason being lack of informed consent. No participants meeting all inclusion and exclusion criteria were excluded from the intention-to-treat analysis. Exclusion of patients was only performed in per-protocol sensitivity analysis. A total of 287 adult patients with acute aneurysmal subarachnoid hemorrhage of all clinical grades were analyzable. Aneurysm treatment with clipping or coiling was performed within 48 hours.
Intervention: A total of 144 patients were randomized to receive an additional lumbar drain after aneurysm treatment and 143 patients to standard of care only. Early lumbar drainage with 5 mL per hour was started within 72 hours of the subarachnoid hemorrhage.
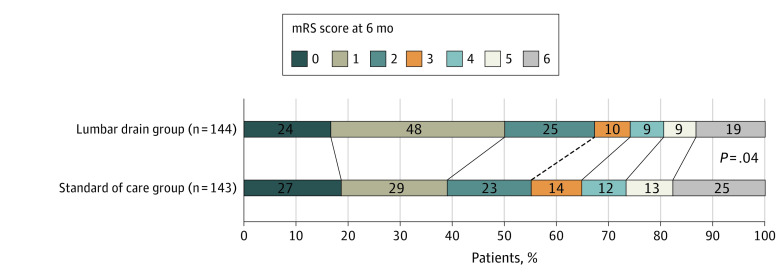
Main outcomes and measures: Primary outcome was the rate of unfavorable outcome, defined as modified Rankin Scale score of 3 to 6 (range, 0 to 6), obtained by masked assessors 6 months after hemorrhage.
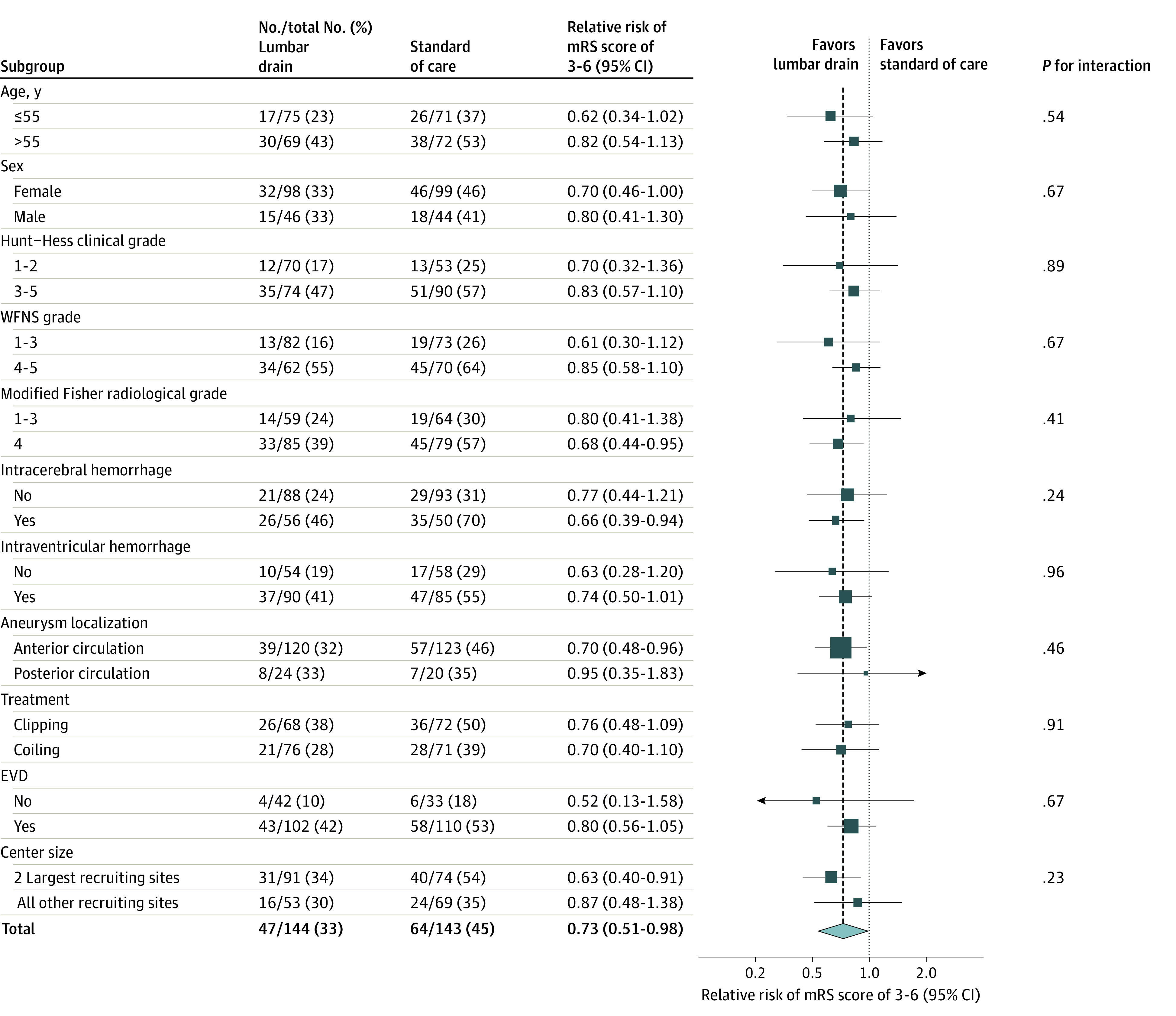
Results: Of 287 included patients, 197 (68.6%) were female, and the median (IQR) age was 55 (48-63) years. Lumbar drainage started at a median (IQR) of day 2 (1-2) after aneurysmal subarachnoid hemorrhage. At 6 months, 47 patients (32.6%) in the lumbar drain group and 64 patients (44.8%) in the standard of care group had an unfavorable neurological outcome (risk ratio, 0.73; 95% CI, 0.52 to 0.98; absolute risk difference, -0.12; 95% CI, -0.23 to -0.01; P = .04). Patients treated with a lumbar drain had fewer secondary infarctions at discharge (41 patients [28.5%] vs 57 patients [39.9%]; risk ratio, 0.71; 95% CI, 0.49 to 0.99; absolute risk difference, -0.11; 95% CI, -0.22 to 0; P = .04).
Conclusion and relevance: In this trial, prophylactic lumbar drainage after aneurysmal subarachnoid hemorrhage lessened the burden of secondary infarction and decreased the rate of unfavorable outcome at 6 months. These findings support the use of lumbar drains after aneurysmal subarachnoid hemorrhage.
Trial registration: ClinicalTrials.gov Identifier: NCT01258257.
Conflict of interest statement
Figures
Comment in
-
Letter to the Editor Regarding "Effectiveness of Cerebrospinal Fluid Lumbar Drainage Among Patients with Aneurysmal Subarachnoid Hemorrhage: An Updated Systematic Review and Meta-Analysis".World Neurosurg. 2024 Jul;187:259-260. doi: 10.1016/j.wneu.2024.04.134. World Neurosurg. 2024. PMID: 38970182 No abstract available.
-
In Reply to the Letter to the Editor Regarding "Effectiveness of Cerebrospinal Fluid Lumbar Drainage Among Patients with Aneurysmal Subarachnoid Hemorrhage: An Updated Systematic Review and Meta-Analysis".World Neurosurg. 2024 Jul;187:261. doi: 10.1016/j.wneu.2024.04.152. World Neurosurg. 2024. PMID: 38970183 No abstract available.
References
-
- Macdonald RL, Higashida RT, Keller E, et al. Clazosentan, an endothelin receptor antagonist, in patients with aneurysmal subarachnoid haemorrhage undergoing surgical clipping: a randomised, double-blind, placebo-controlled phase 3 trial (CONSCIOUS-2). Lancet Neurol. 2011;10(7):618-625. doi: 10.1016/S1474-4422(11)70108-9 - DOI - PubMed
