

Global, regional, and national prevalence and mortality burden of sickle cell disease, 2000-2021: a systematic analysis from the Global Burden of Disease Study 2021
- PMID: 37331373
- PMCID: PMC10390339
- DOI: 10.1016/S2352-3026(23)00118-7
Global, regional, and national prevalence and mortality burden of sickle cell disease, 2000-2021: a systematic analysis from the Global Burden of Disease Study 2021
Erratum in
-
Correction to Lancet Haematol 2023; 10: e585-99.Lancet Haematol. 2023 Aug;10(8):e574. doi: 10.1016/S2352-3026(23)00215-6. Lancet Haematol. 2023. PMID: 37532415 Free PMC article. No abstract available.
Abstract
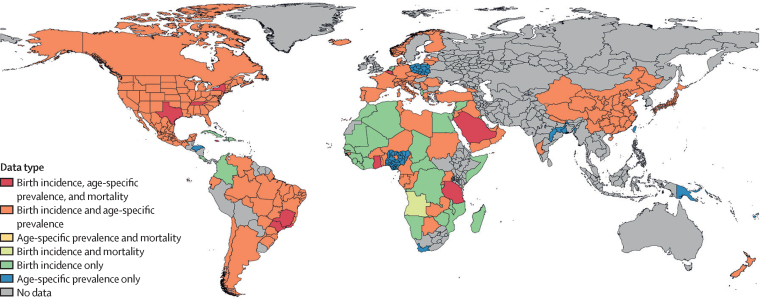
Background: Previous global analyses, with known underdiagnosis and single cause per death attribution systems, provide only a small insight into the suspected high population health effect of sickle cell disease. Completed as part of the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2021, this study delivers a comprehensive global assessment of prevalence of sickle cell disease and mortality burden by age and sex for 204 countries and territories from 2000 to 2021.
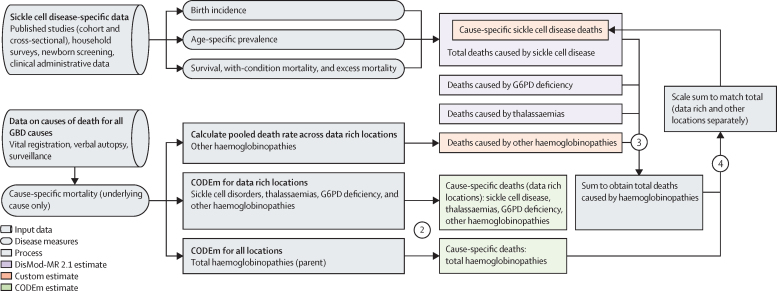
Methods: We estimated cause-specific sickle cell disease mortality using standardised GBD approaches, in which each death is assigned to a single underlying cause, to estimate mortality rates from the International Classification of Diseases (ICD)-coded vital registration, surveillance, and verbal autopsy data. In parallel, our goal was to estimate a more accurate account of sickle cell disease health burden using four types of epidemiological data on sickle cell disease: birth incidence, age-specific prevalence, with-condition mortality (total deaths), and excess mortality (excess deaths). Systematic reviews, supplemented with ICD-coded hospital discharge and insurance claims data, informed this modelling approach. We employed DisMod-MR 2.1 to triangulate between these measures-borrowing strength from predictive covariates and across age, time, and geography-and generated internally consistent estimates of incidence, prevalence, and mortality for three distinct genotypes of sickle cell disease: homozygous sickle cell disease and severe sickle cell β-thalassaemia, sickle-haemoglobin C disease, and mild sickle cell β-thalassaemia. Summing the three models yielded final estimates of incidence at birth, prevalence by age and sex, and total sickle cell disease mortality, the latter of which was compared directly against cause-specific mortality estimates to evaluate differences in mortality burden assessment and implications for the Sustainable Development Goals (SDGs).
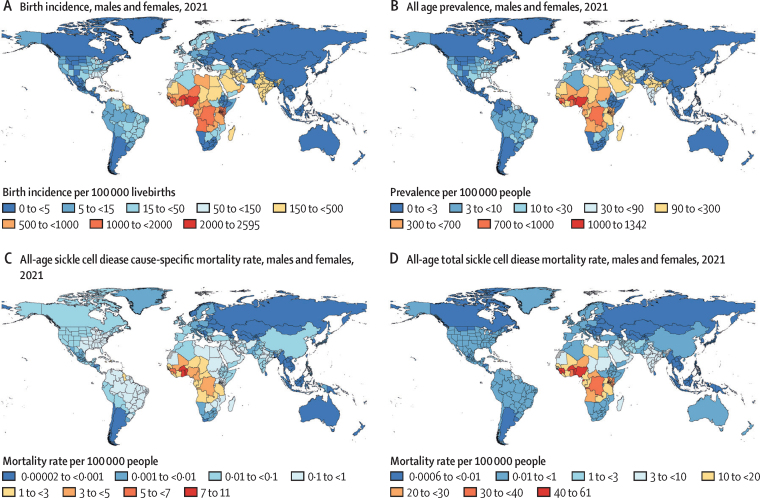
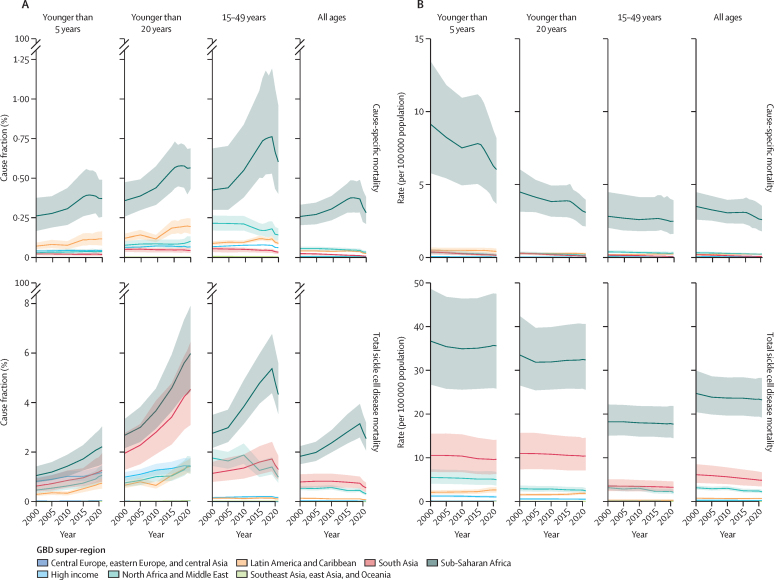
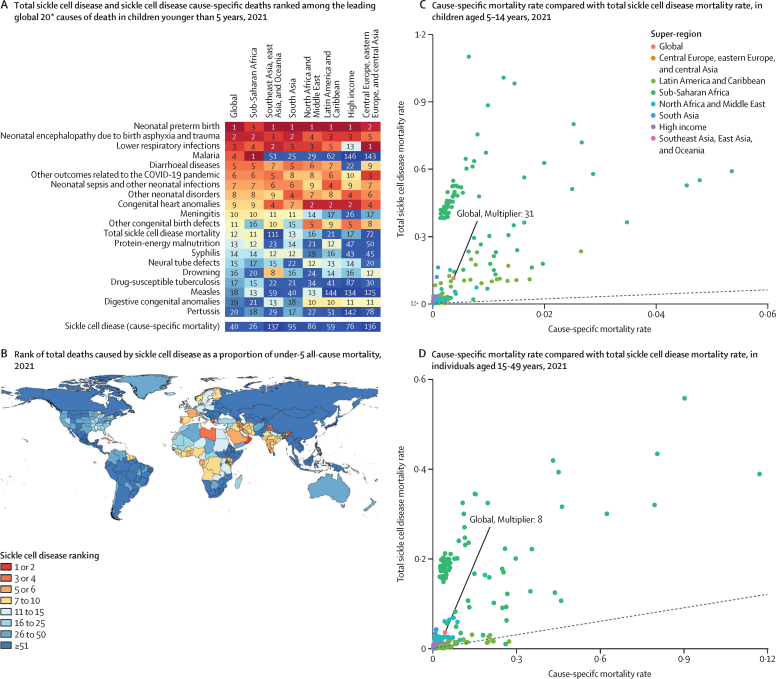
Findings: Between 2000 and 2021, national incidence rates of sickle cell disease were relatively stable, but total births of babies with sickle cell disease increased globally by 13·7% (95% uncertainty interval 11·1-16·5), to 515 000 (425 000-614 000), primarily due to population growth in the Caribbean and western and central sub-Saharan Africa. The number of people living with sickle cell disease globally increased by 41·4% (38·3-44·9), from 5·46 million (4·62-6·45) in 2000 to 7·74 million (6·51-9·2) in 2021. We estimated 34 400 (25 000-45 200) cause-specific all-age deaths globally in 2021, but total sickle cell disease mortality burden was nearly 11-times higher at 376 000 (303 000-467 000). In children younger than 5 years, there were 81 100 (58 800-108 000) deaths, ranking total sickle cell disease mortality as 12th (compared to 40th for cause-specific sickle cell disease mortality) across all causes estimated by the GBD in 2021.
Interpretation: Our findings show a strikingly high contribution of sickle cell disease to all-cause mortality that is not apparent when each death is assigned to only a single cause. Sickle cell disease mortality burden is highest in children, especially in countries with the greatest under-5 mortality rates. Without comprehensive strategies to address morbidity and mortality associated with sickle cell disease, attainment of SDG 3.1, 3.2, and 3.4 is uncertain. Widespread data gaps and correspondingly high uncertainty in the estimates highlight the urgent need for routine and sustained surveillance efforts, further research to assess the contribution of conditions associated with sickle cell disease, and widespread deployment of evidence-based prevention and treatment for those with sickle cell disease.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2023 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests L M Force reports support for this Article from the Bill & Melinda Gates Foundation; grants or contracts from Conquer Cancer Foundation, St Jude Children's Research Hospital, St Baldrick's Foundation, and National Institutes of Health (NIH) Loan Repayment Program; leadership or fiduciary roles in board, society, committee or advocacy groups, unpaid with Lancet Oncology International Advisory Board, outside the submitted work. K Fuller reports support for this Article from the Institute for Health Metrics and Evaluation and the Gates Foundation. P Gill reports other support as a National Institute for Health and Care Research (NIHR) Senior Investigator; the views expressed in this publication are those of the author and not necessarily those of the NIHR or the UK Department of Health and Social Care; all outside the submitted work. N J Kassebaum reports grant funding support for this Article from the Gates Foundation. K Kewal reports other non-financial support from UGC Centre of Advanced Study, CAS II, Department of Anthropology, Panjab University, Chandigarh, India; all outside the submitted work. F B Piel reports grants or contracts from the National Health Service Race and Health Observatory; consulting fees from Bluebird Bio; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from King's Sickle Cell Preceptorship 2023; support for attending meetings or travel from 4th Global Sickle Cell Disease Congress; participation on a data safety monitoring board or advisory board with Fondation Pierre Fabre; all outside the submitted work. J A Singh reports consulting fees from Crealta/Horizon, Medisys, Fidia, PK Med, Two labs, Adept Field Solutions, Clinical Care Options, ClearView Healthcare Partners, Putnam Associates, Focus Forward, Navigant Consulting, Spherix, MedIQ, Jupiter Life Science, UBM, Trio Health, Medscape, WebMD, and Practice Point Communications; and the NIH and the American College of Rheumatology; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from the speaker's bureau of Simply Speaking; support for attending meetings or travel from the steering committee of OMERACT; participation on a data safety monitoring board or advisory board as a member of the US Food and Drug Administration Arthritis Advisory Committee; leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid with OMERACT as a steering committee member; leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid with the Veterans Affairs of Rheumatology Field Advisory Committee as a chair; leadership or fiduciary roles in board, society, committee or advocacy groups, paid or unpaid with UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis as the editor and director; stock or stock options in TPT Global Tech, Vaxart Pharmaceuticals, Atyu Biopharma, Adaptimmune Therapeutics, GeoVax Labs, Pieris Pharmaceuticals, Enzolytics, Seres Therapeutics, Tonix Pharmaceuticals, and Charlotte's Web Holdings, with previously owned stock options in Amarin, Viking, and Moderna Pharmaceuticals; all outside the submitted work.
Figures
Comment in
-
Sickle cell disease: time to act on the most neglected global health problem.Lancet Haematol. 2023 Aug;10(8):e558-e559. doi: 10.1016/S2352-3026(23)00169-2. Epub 2023 Jun 15. Lancet Haematol. 2023. PMID: 37331372 No abstract available.
References
-
- Williams TN, Obaro SK. Sickle cell disease and malaria morbidity: a tale with two tails. Trends Parasitol. 2011;27:315–320. - PubMed
-
- Kauf TL, Coates TD, Huazhi L, Mody-Patel N, Hartzema AG. The cost of health care for children and adults with sickle cell disease. Am J Hematol. 2009;84:323–327. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
