

Theranostics and Patient-Specific Dosimetry
- PMID: 37331786
- PMCID: PMC10414757
- DOI: 10.1016/j.semradonc.2023.03.011
Theranostics and Patient-Specific Dosimetry
Abstract
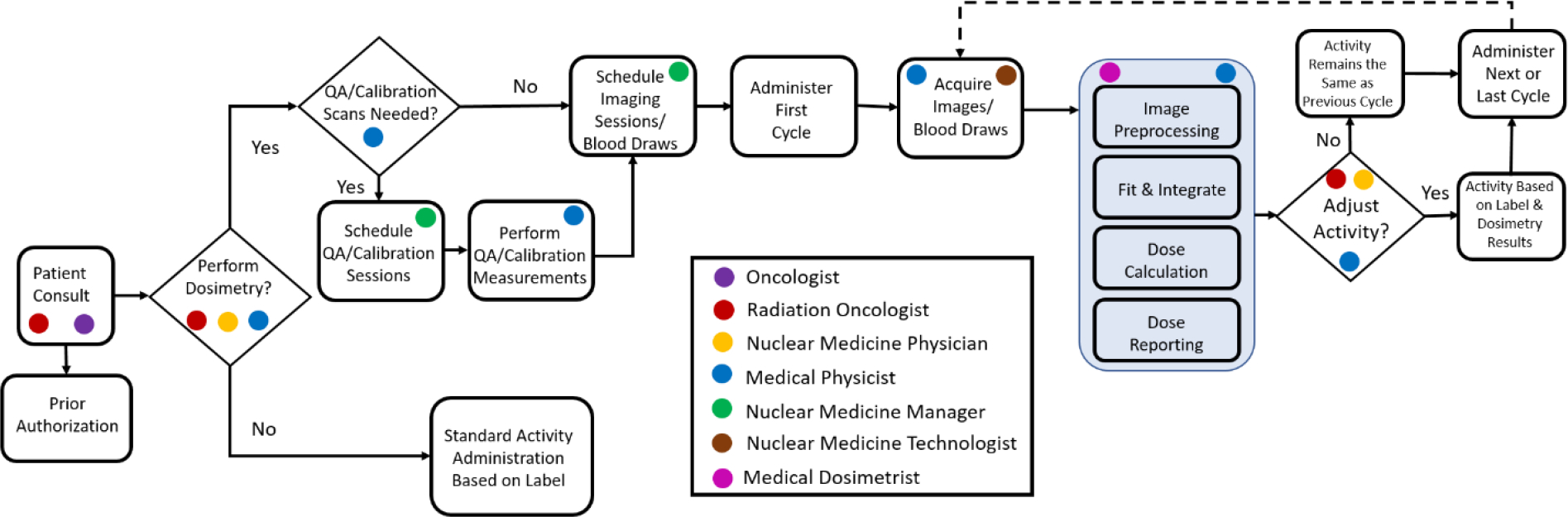
Radiopharmaceutical therapy (RPT) is an invigorated form of cancer therapy that systemically delivers targeted radioactive drugs to cancer cells. Theranostics is a type of RPT that utilizes imaging, either of the RPT drug directly or a companion diagnostic, to inform whether a patient will benefit from the treatment. Given the ability to image the drug onboard theranostic treatments also lends itself readily to patient-specific dosimetry, which is a physics-based process that determines the overall absorbed dose burden to healthy organs and tissues and tumors in patients. While companion diagnostics identify who will benefit from RPT treatments, dosimetry determines how much activity these beneficiaries can receive to maximize therapeutic efficacy. Clinical data is starting to accrue suggesting tremendous benefits when dosimetry is performed for RPT patients. RPT dosimetry, which was once performed by florid and often inaccurate workflows, can now be performed more efficiently and accurately with FDA-cleared dosimetry software. Therefore, there is no better time for the field of oncology to adopt this form of personalize medicine to improve outcomes for cancer patients.
Copyright © 2023 Elsevier Inc. All rights reserved.
Conflict of interest statement
COI Statement: Bryan Bednarz is Chairman and CSO of Voximetry, Inc a nuclear medicine dosimetry company located in Middleton, WI and has financial interest in the company.
Figures




References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
