

Detection of pneumococcus during hospitalization for SARS-CoV-2
- PMID: 37332510
- PMCID: PMC10117745
- DOI: 10.1093/femsmc/xtac026
Detection of pneumococcus during hospitalization for SARS-CoV-2
Abstract
Background: Infections with respiratory viruses [e.g. influenza and respiratory syncytial virus (RSV)] can increase the risk of severe pneumococcal infections. Likewise, pneumococcal coinfection is associated with poorer outcomes in viral respiratory infection. However, there are limited data describing the frequency of pneumococcus and SARS-CoV-2 coinfection and the role of coinfection in influencing COVID-19 severity. We, therefore, investigated the detection of pneumococcus in COVID-19 inpatients during the early pandemic period.
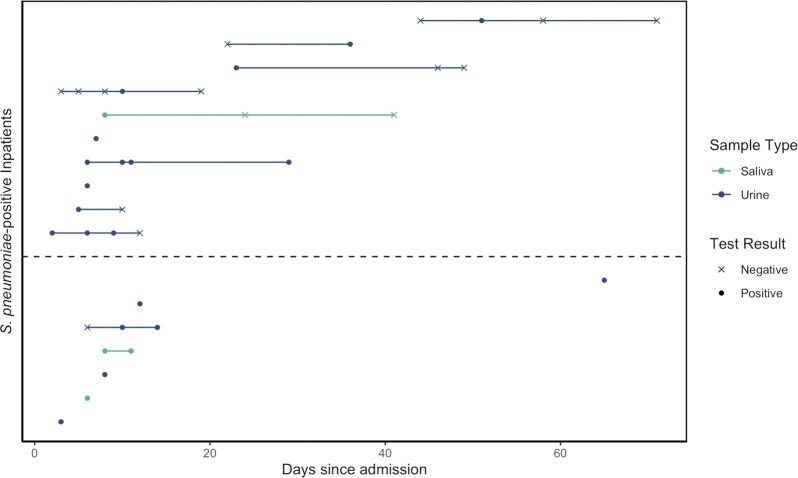
Methods: The study included patients aged 18 years and older, admitted to the Yale-New Haven Hospital who were symptomatic for respiratory infection and tested positive for SARS-CoV-2 during March-August 2020. Patients were tested for pneumococcus through culture-enrichment of saliva followed by RT-qPCR (to identify carriage) and serotype-specific urine antigen detection (UAD) assays (to identify presumed lower respiratory tract pneumococcal disease).
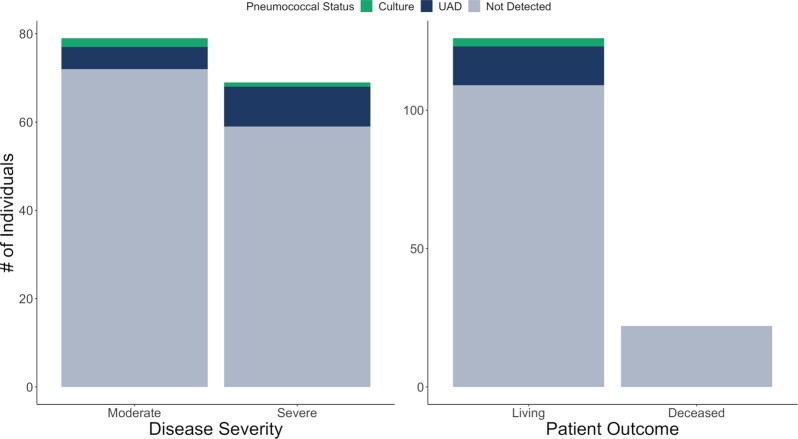
Results: Among 148 subjects, the median age was 65 years; 54.7% were male; 50.7% had an ICU stay; 64.9% received antibiotics; and 14.9% died while admitted. Pneumococcal carriage was detected in 3/96 (3.1%) individuals tested by saliva RT-qPCR. Additionally, pneumococcus was detected in 14/127 (11.0%) individuals tested by UAD, and more commonly in severe than moderate COVID-19 [OR: 2.20; 95% CI: (0.72, 7.48)]; however, the numbers were small with a high degree of uncertainty. None of the UAD-positive individuals died.
Conclusions: Pneumococcal lower respiratory tract infection (LRTI), as detected by positive UAD, occurred in patients hospitalized with COVID-19. Moreover, pneumococcal LRTI was more common in those with more serious COVID-19 outcomes. Future studies should assess how pneumococcus and SARS-CoV-2 interact to influence COVID-19 severity in hospitalized patients.
Keywords: COVID-19; Streptococcus pneumoniae; saliva; urinary antigen detection.
© The Author(s) 2022. Published by Oxford University Press on behalf of FEMS.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous