

Sequential disruptions to inflammatory and angiogenic pathways and risk of spontaneous preterm birth in Malawian women
- PMID: 37332611
- PMCID: PMC10275952
- DOI: 10.1016/j.isci.2023.106912
Sequential disruptions to inflammatory and angiogenic pathways and risk of spontaneous preterm birth in Malawian women
Abstract
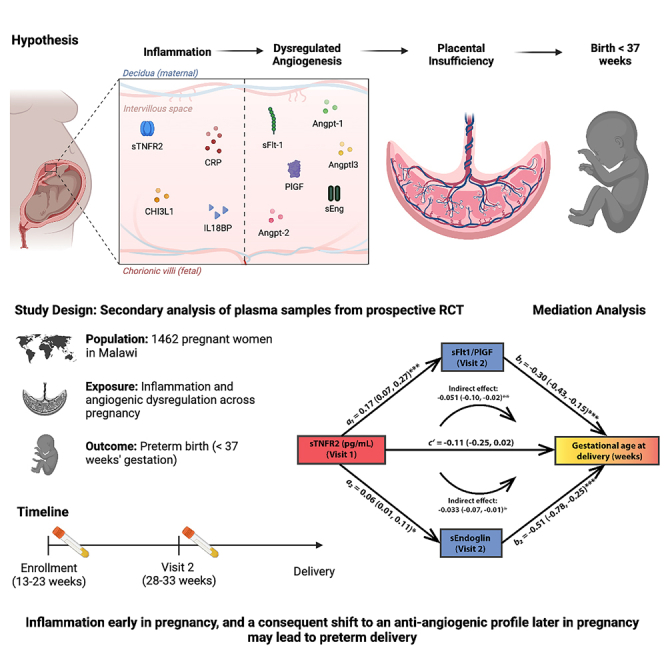
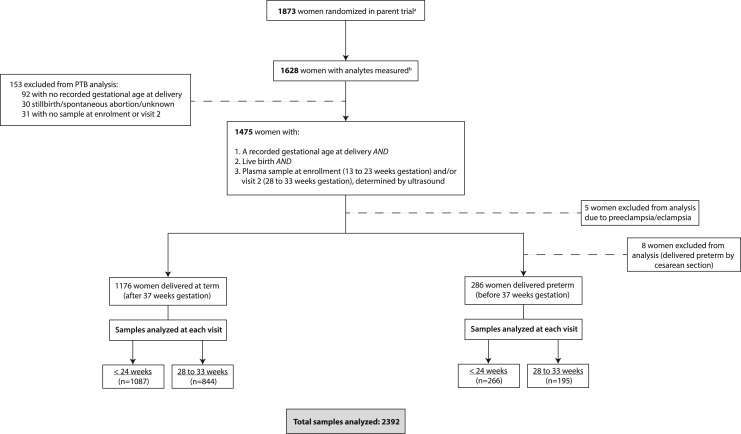
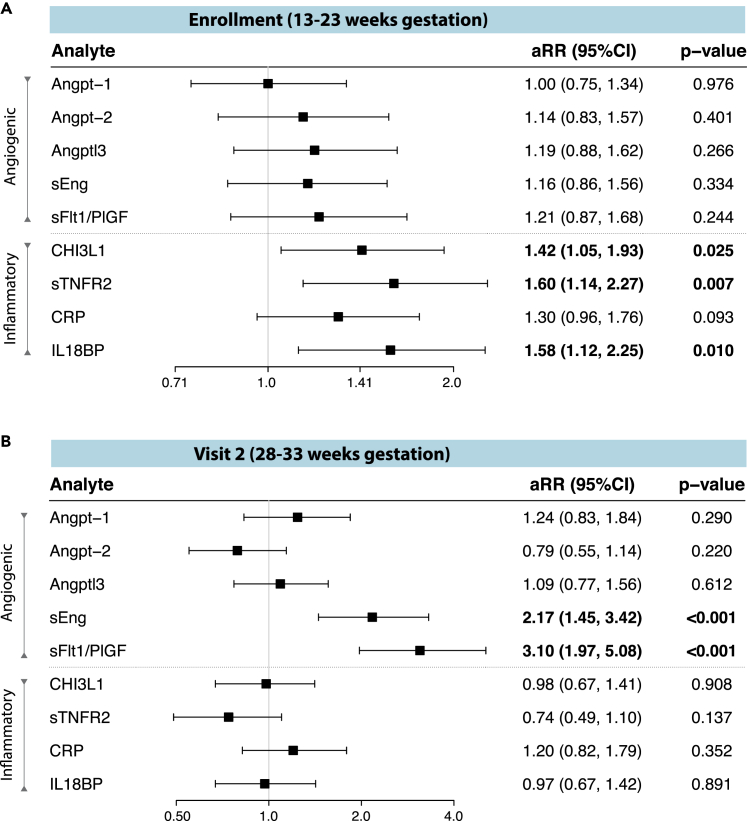
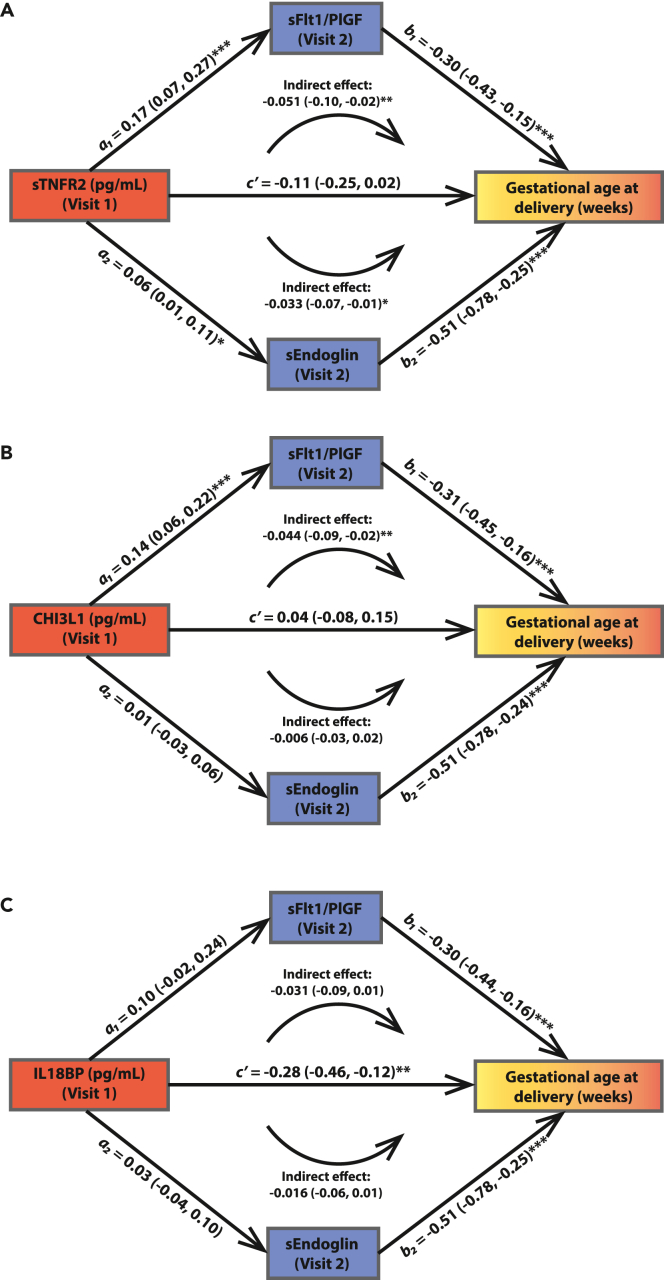
Preterm birth is a leading cause of death in children under five years of age. We hypothesized that sequential disruptions to inflammatory and angiogenic pathways during pregnancy increase the risk of placental insufficiency and spontaneous preterm labor and delivery. We conducted a secondary analysis of inflammatory and angiogenic analytes measured in plasma samples collected across pregnancy from 1462 Malawian women. Women with concentrations of the inflammatory markers sTNFR2, CHI3L1, and IL18BP in the highest quartile before 24 weeks gestation and women with anti-angiogenic factors sEndoglin and sFlt-1/PlGF ratio in the highest quartile at 28-33 weeks gestation had an increased relative risk of preterm birth. Mediation analysis further supported a potential causal link between early inflammation, subsequent angiogenic dysregulation detrimental to placental vascular development, and earlier gestational age at delivery. Interventions designed to reduce the burden of preterm birth may need to be implemented before 24 weeks of gestation.
Keywords: Clinical finding; Health sciences; Pregnancy.
Crown Copyright © 2023.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
The use of angiogenic biomarkers in maternal blood to identify which SGA fetuses will require a preterm delivery and mothers who will develop pre-eclampsia.J Matern Fetal Neonatal Med. 2016;29(8):1214-28. doi: 10.3109/14767058.2015.1048431. J Matern Fetal Neonatal Med. 2016. PMID: 26303962 Free PMC article.
-
Inflammatory and Angiogenic Factors at Mid-Pregnancy Are Associated with Spontaneous Preterm Birth in a Cohort of Tanzanian Women.PLoS One. 2015 Aug 6;10(8):e0134619. doi: 10.1371/journal.pone.0134619. eCollection 2015. PLoS One. 2015. PMID: 26247200 Free PMC article.
-
Early pregnancy maternal and fetal angiogenic factors and fetal and childhood growth: the Generation R Study.Hum Reprod. 2015 Jun;30(6):1302-13. doi: 10.1093/humrep/dev070. Epub 2015 Apr 8. Hum Reprod. 2015. PMID: 25854264
-
Combining Biomarkers to Predict Pregnancy Complications and Redefine Preeclampsia: The Angiogenic-Placental Syndrome.Hypertension. 2020 Apr;75(4):918-926. doi: 10.1161/HYPERTENSIONAHA.119.13763. Epub 2020 Feb 17. Hypertension. 2020. PMID: 32063058 Free PMC article. Review.
-
Clinical utility of sFlt-1 and PlGF in screening, prediction, diagnosis and monitoring of pre-eclampsia and fetal growth restriction.Ultrasound Obstet Gynecol. 2023 Feb;61(2):168-180. doi: 10.1002/uog.26032. Ultrasound Obstet Gynecol. 2023. PMID: 35816445 Review.
Cited by
-
Tracing neurodevelopment and growth pattern in six-year-old children with idiopathic clubfoot: a national cohort study.BMC Musculoskelet Disord. 2025 Jun 2;26(1):542. doi: 10.1186/s12891-025-08810-w. BMC Musculoskelet Disord. 2025. PMID: 40457287 Free PMC article.
References
-
- Liu L., Oza S., Hogan D., Chu Y., Perin J., Zhu J., Lawn J.E., Cousens S., Mathers C., Black R.E. Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet. 2016;388:3027–3035. doi: 10.1016/S0140-6736(16)31593-8. - DOI - PMC - PubMed
-
- Blencowe H., Cousens S., Oestergaard M.Z., Chou D., Moller A.B., Narwal R., Adler A., Vera Garcia C., Rohde S., Say L., Lawn J.E. National , regional , and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries : a systematic analysis and implications. Lancet. 2012;379:2162–2172. doi: 10.1016/S0140-6736(12)60820-4. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
