

Genetic Movement Disorders Commonly Seen in Asians
- PMID: 37332644
- PMCID: PMC10272919
- DOI: 10.1002/mdc3.13737
Genetic Movement Disorders Commonly Seen in Asians
Abstract
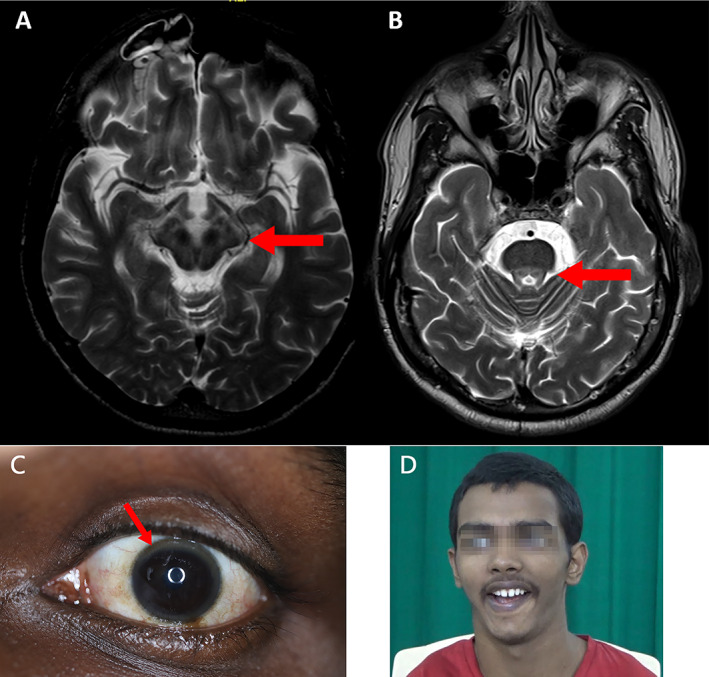
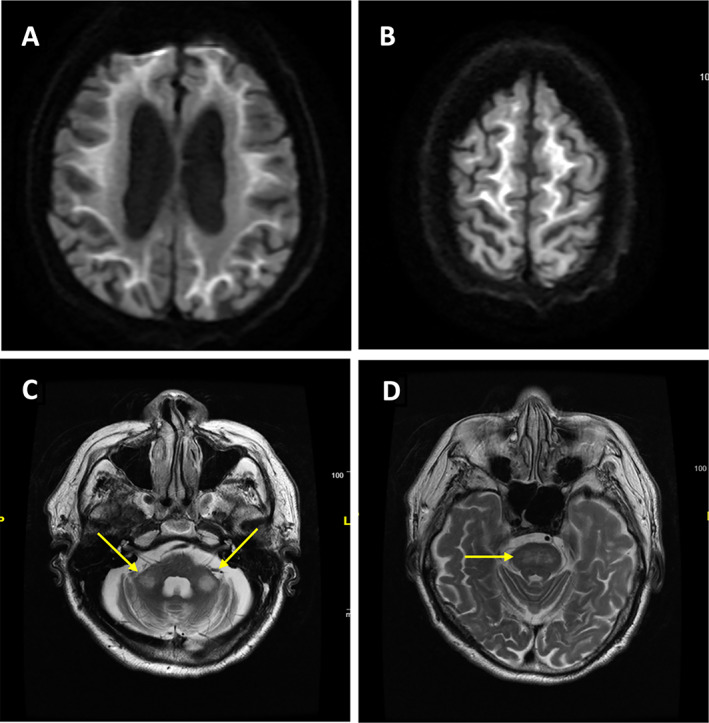
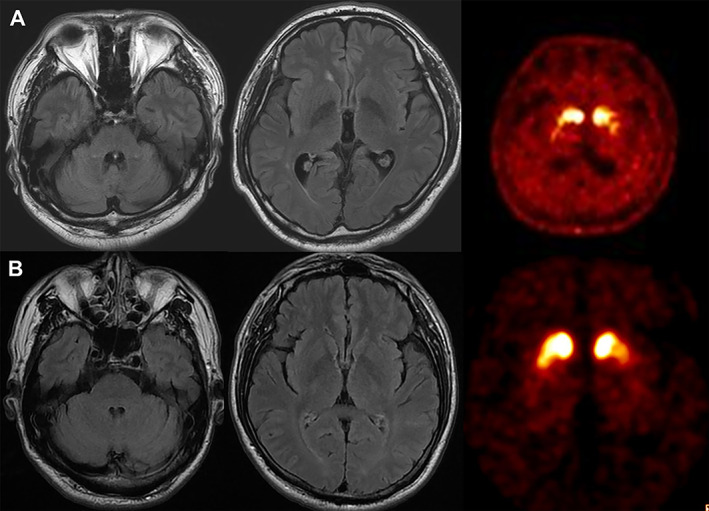
The increasing availability of molecular genetic testing has changed the landscape of both genetic research and clinical practice. Not only is the pace of discovery of novel disease-causing genes accelerating but also the phenotypic spectra associated with previously known genes are expanding. These advancements lead to the awareness that some genetic movement disorders may cluster in certain ethnic populations and genetic pleiotropy may result in unique clinical presentations in specific ethnic groups. Thus, the characteristics, genetics and risk factors of movement disorders may differ between populations. Recognition of a particular clinical phenotype, combined with information about the ethnic origin of patients could lead to early and correct diagnosis and assist the development of future personalized medicine for patients with these disorders. Here, the Movement Disorders in Asia Task Force sought to review genetic movement disorders that are commonly seen in Asia, including Wilson's disease, spinocerebellar ataxias (SCA) types 12, 31, and 36, Gerstmann-Sträussler-Scheinker disease, PLA2G6-related parkinsonism, adult-onset neuronal intranuclear inclusion disease (NIID), and paroxysmal kinesigenic dyskinesia. We also review common disorders seen worldwide with specific mutations or presentations that occur frequently in Asians.
Keywords: Asia; genetic; movement disorders.
© 2023 International Parkinson and Movement Disorder Society.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
