

Modified hypoglossal-facial nerve anastomosis for peripheral-type facial palsy caused by pontine infarction: A case report and literature review
- PMID: 37332903
- PMCID: PMC10275953
- DOI: 10.1016/j.heliyon.2023.e16909
Modified hypoglossal-facial nerve anastomosis for peripheral-type facial palsy caused by pontine infarction: A case report and literature review
Abstract
Background: Peripheral-type facial palsy could be caused by a lesion in the tegmentum of the pons, such as infarction, with a rare occurrence. We herein described a case of unilateral peripheral-type facial palsy induced by dorsolateral pontine infarction and treated this patient using modified hypoglossal-facial nerve anastomosis.
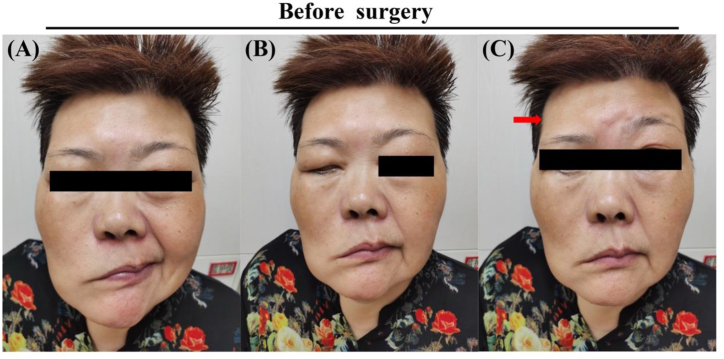
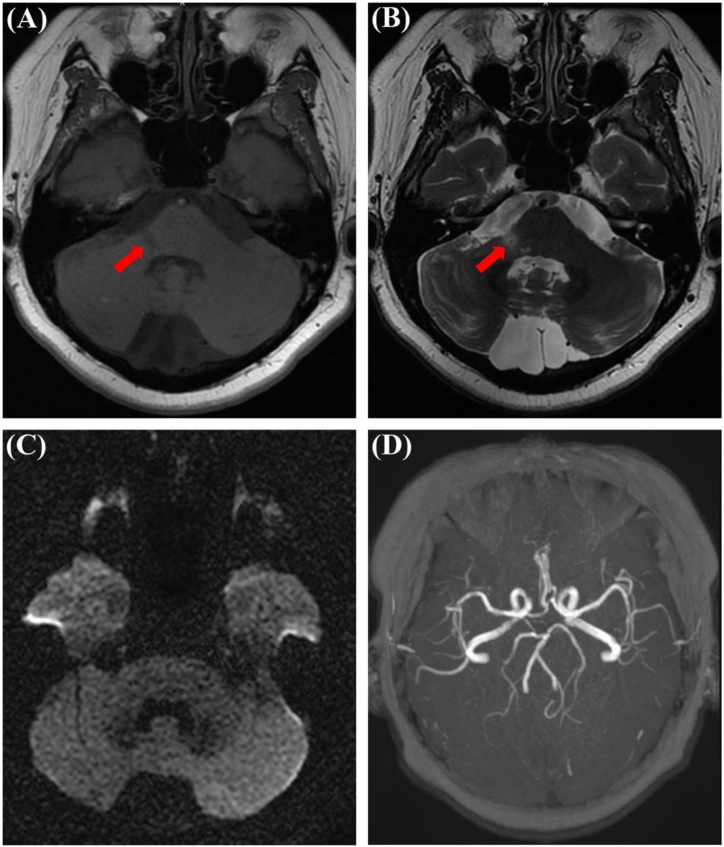
Case presentation: A 60-year-old female presented with dizziness, hearing drop, diplopia, and peripheral-type facial palsy. Brain Magnetic Resonance Imaging showed a dorsolateral pontine infarction on the right side which exactly refers to the location of the ipsilateral facial nucleus or facial nerve fascicles at the pons. Subsequent electrophysiological examinations confirmed poor facial nerve function of this patient and modified hypoglossal-facial nerve anastomosis was then performed.
Conclusions: This case reminded medical practitioners not to ignore the possibility of involvement of a central cause in peripheral-type facial palsy patients. In addition, modified hypoglossal-facial nerve anastomosis served as a useful skill improvement that may help reduce hemiglossal dysfunction while restoring facial muscle function.
Keywords: Case report; Nerve anastomosis; Peripheral-type facial palsy; Pontine infarction.
© 2023 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


References
-
- Hebant B., et al. Isolated peripheral-type facial palsy due to contralateral precentral gyrus cavernoma hemorrhage. J. Clin. Neurosci. 2020;72:452–453. - PubMed
-
- Park J.H., Yoo H.U., Shin H.W. Peripheral type facial palsy in a patient with dorsolateral medullary infarction with infranuclear involvement of the caudal pons. J. Stroke Cerebrovasc. Dis. 2008;17(5):263–265. - PubMed
-
- Luijmes R.E., et al. Quality of life before and after different treatment modalities in peripheral facial palsy: a systematic review. Laryngoscope. 2017;127(5):1044–1051. - PubMed
-
- Guntinas-Lichius O. The facial nerve in the presence of a head and neck neoplasm: assessment and outcome after surgical management. Curr. Opin. Otolaryngol. Head Neck Surg. 2004;12(2):133–141. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
