

Primary motor hand area corticospinal excitability indicates overall functional recovery after spinal cord injury
- PMID: 37333013
- PMCID: PMC10273270
- DOI: 10.3389/fneur.2023.1175078
Primary motor hand area corticospinal excitability indicates overall functional recovery after spinal cord injury
Abstract
Background: After spinal cord injury (SCI), the excitability of the primary motor cortex (M1) lower extremity area decreases or disappears. A recent study reported that the M1 hand area of the SCI patient encodes the activity information of both the upper and lower extremities. However, the characteristics of the M1 hand area corticospinal excitability (CSE) changes after SCI and its correlation with extremities motor function are still unknown.
Methods: A retrospective study was conducted on the data of 347 SCI patients and 80 healthy controls on motor evoked potentials (MEP, reflection of CSE), extremity motor function, and activities of daily living (ADL) ability. Correlation analysis and multiple linear regression analysis were conducted to analyze the relationship between the degree of MEP hemispheric conversion and extremity motor function/ADL ability.
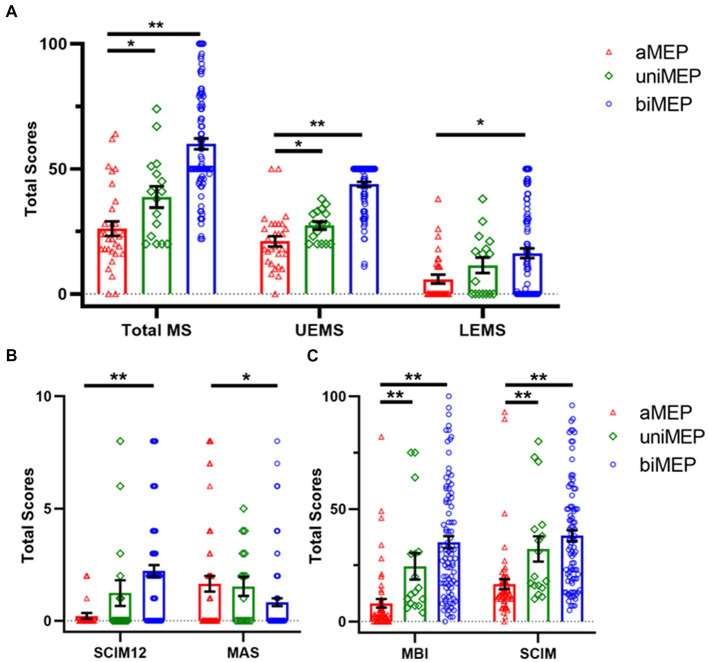
Results: The CSE of the dominant hemisphere M1 hand area decreased in SCI patients. In 0-6 m, AIS A grade, or non-cervical injury SCI patients, the degree of M1 hand area MEP hemispheric conversion was positively correlated with total motor score, lower extremity motor score (LEMS), and ADL ability. Multiple linear regression analysis further confirmed the contribution of MEP hemispheric conversion degree in ADL changes as an independent factor.
Conclusion: The closer the degree of M1 hand area MEP hemispheric conversion is to that of healthy controls, the better the extremity motor function/ADL ability patients achieve. Based on the law of this phenomenon, targeted intervention to regulate the excitability of bilateral M1 hand areas might be a novel strategy for SCI overall functional recovery.
Keywords: ADL; MEP; corticospinal excitability; motor function; spinal cord injury.
Copyright © 2023 Dai, Gao, Lin, Xue, Liang, Xu, Wu, Cheng, Hu, Zhao, Yuan and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures





References
-
- Krogh S, Aagaard P, Jønsson AB, Figlewski K, Kasch H. Effects of repetitive transcranial magnetic stimulation on recovery in lower limb muscle strength and gait function following spinal cord injury: a randomized controlled trial. Spinal Cord. (2022) 60:135–41. doi: 10.1038/s41393-021-00703-8, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources