

This is a preprint.
Low-Field Combined Diffusion-Relaxation MRI for Mapping Placenta Structure and Function
- PMID: 37333076
- PMCID: PMC10274995
- DOI: 10.1101/2023.06.06.23290983
Low-Field Combined Diffusion-Relaxation MRI for Mapping Placenta Structure and Function
Abstract
Purpose: Demonstrating quantitative multi-parametric mapping in the placenta with combined -diffusion MRI at low-field (0.55T).
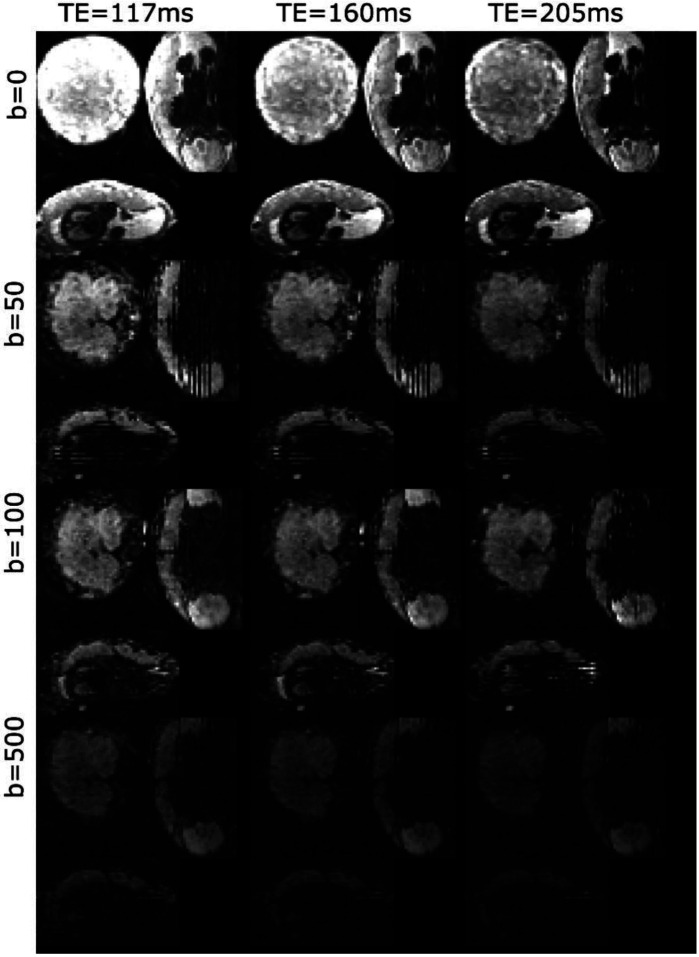
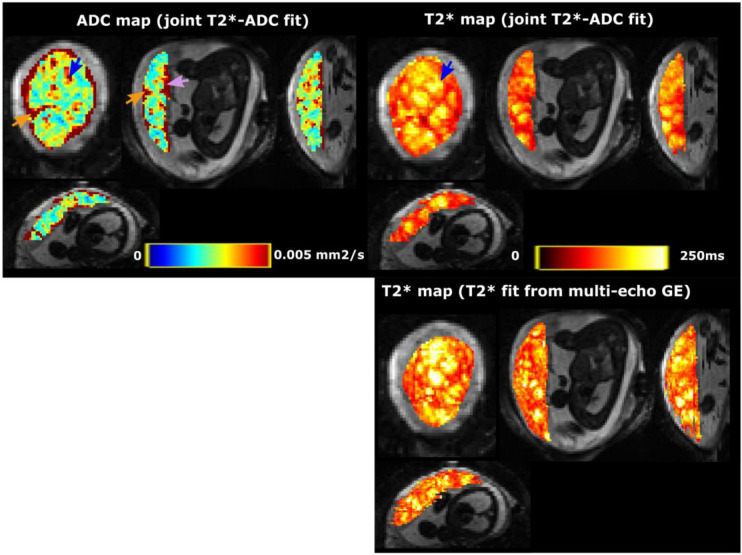
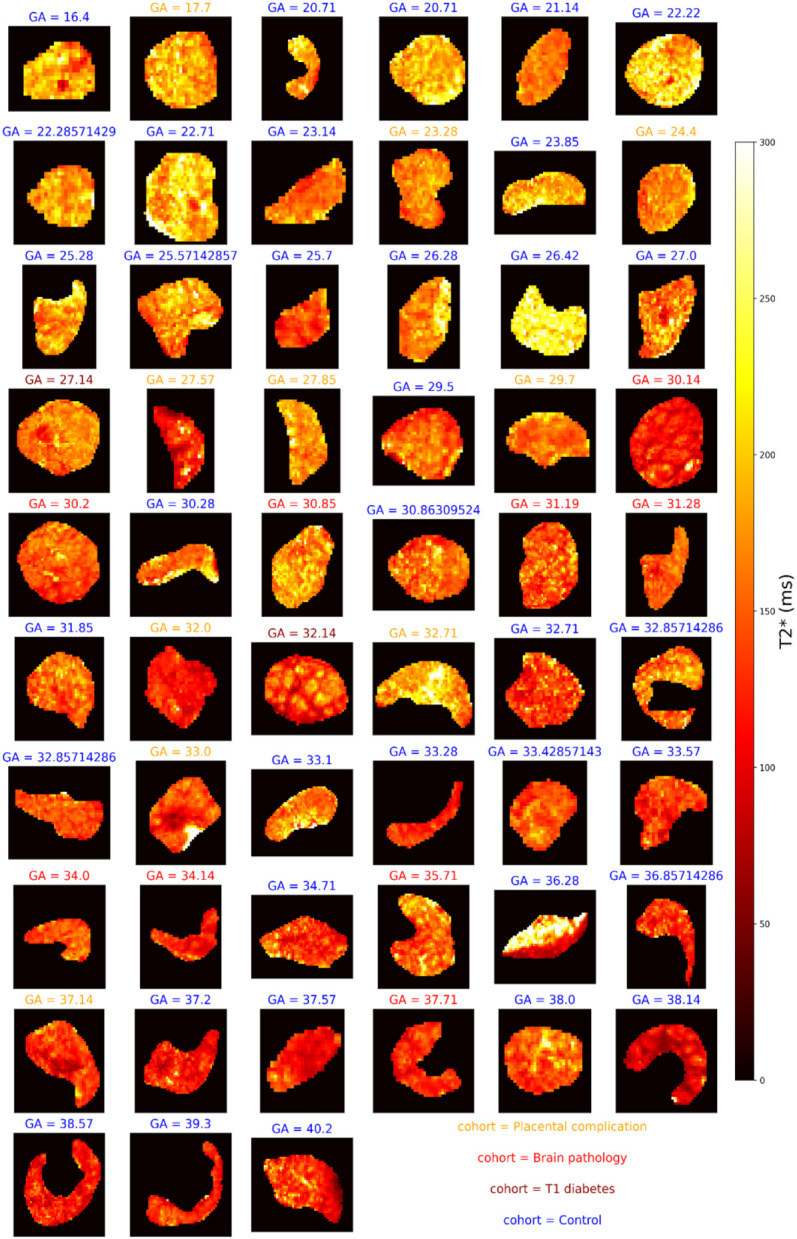
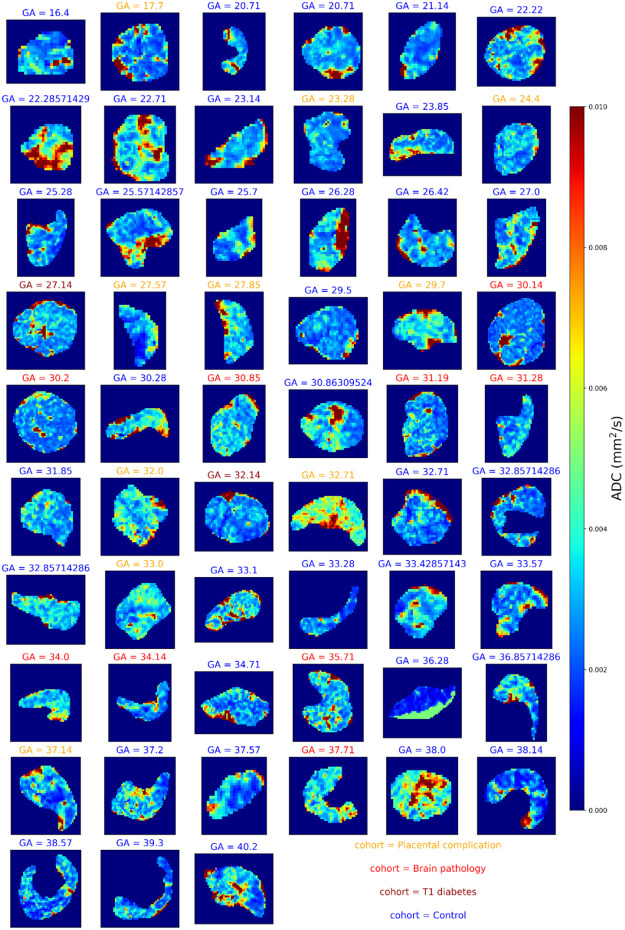
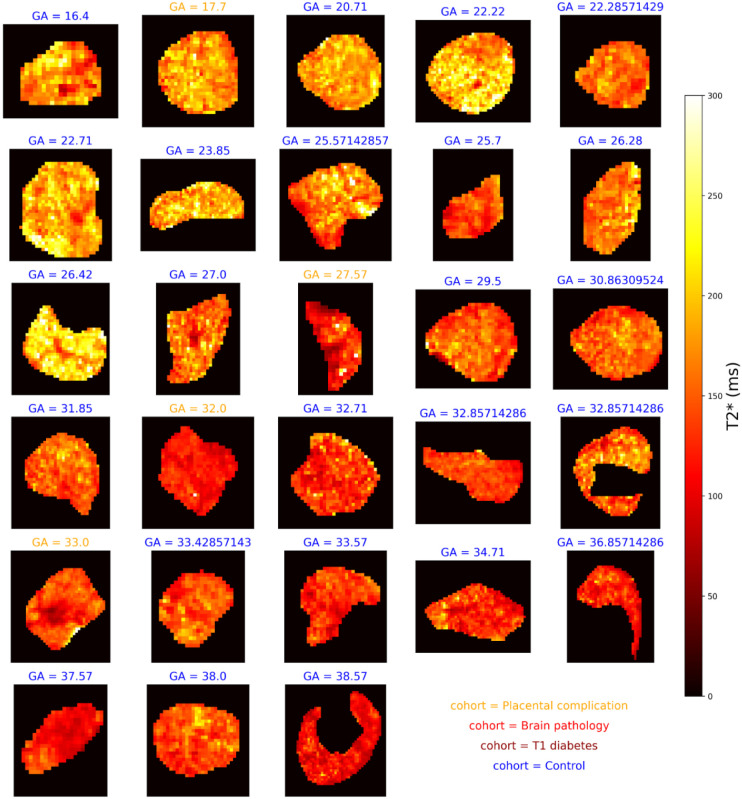
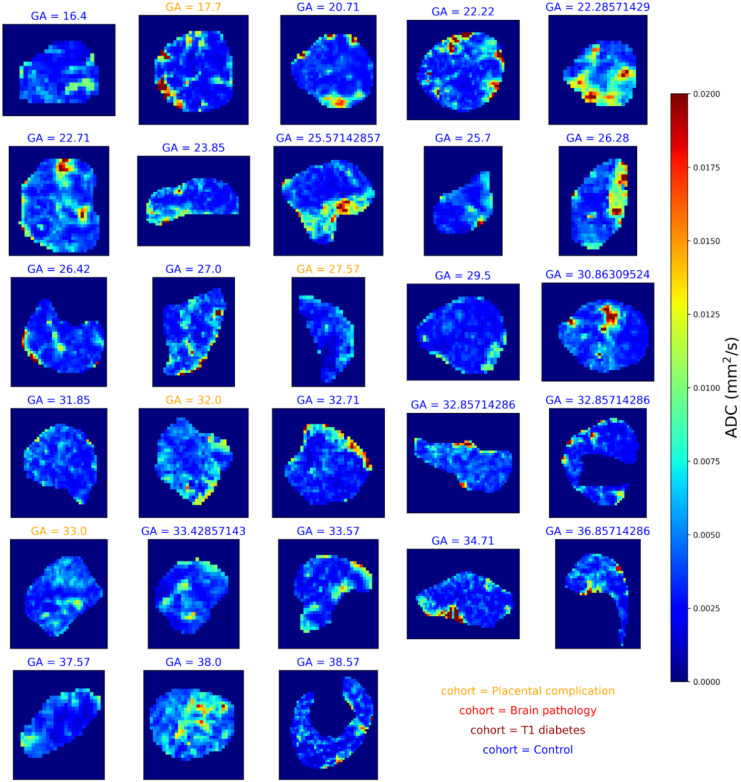
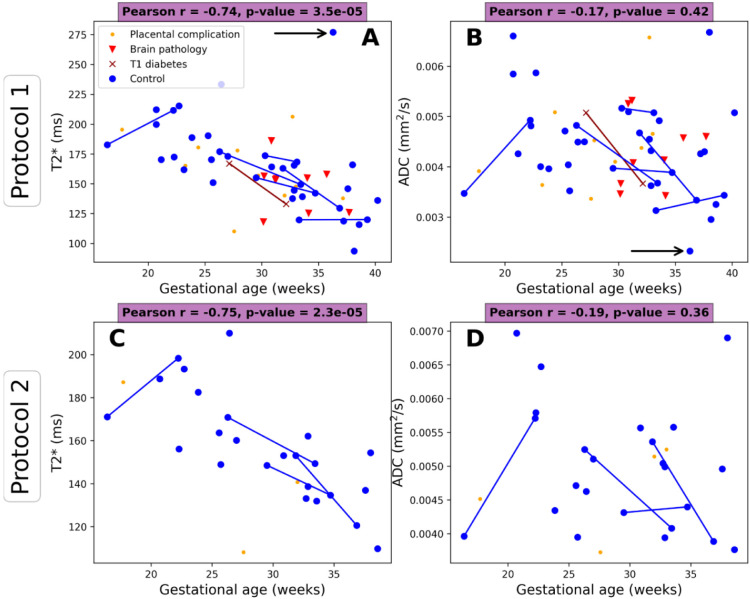
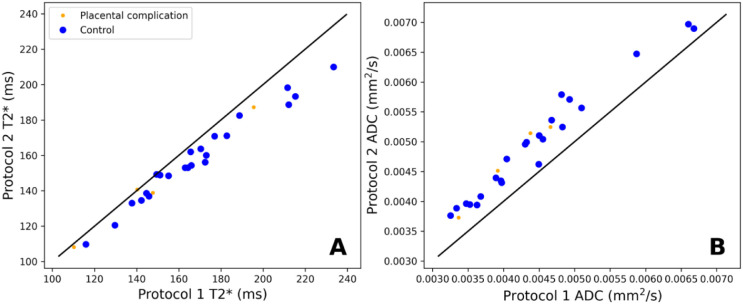
Methods: We present 57 placental MRI scans performed on a commercially available 0.55T scanner. We acquired the images using a combined -diffusion technique scan that simultaneously acquires multiple diffusion preparations and echo times. We processed the data to produce quantitative and diffusivity maps using a combined -ADC model. We compared the derived quantitative parameters across gestation in healthy controls and a cohort of clinical cases.
Results: Quantitative parameter maps closely resemble those from previous experiments at higher field strength, with similar trends in and ADC against gestational age observed.
Conclusion: Combined -diffusion placental MRI is reliably achievable at 0.55T. The advantages of lower field strength - such as cost, ease of deployment, increased accessibility and patient comfort due to the wider bore, and increased for larger dynamic ranges - can support the widespread roll out of placental MRI as an adjunct to ultrasound during pregnancy.
Figures
Similar articles
-
Placental T2* as a measure of placental function across field strength from 0.55T to 3T.Sci Rep. 2024 Nov 19;14(1):28594. doi: 10.1038/s41598-024-77406-6. Sci Rep. 2024. PMID: 39562648 Free PMC article.
-
Reliability and Feasibility of Low-Field-Strength Fetal MRI at 0.55 T during Pregnancy.Radiology. 2023 Oct;309(1):e223050. doi: 10.1148/radiol.223050. Radiology. 2023. PMID: 37847139 Free PMC article.
-
Characterizing T1 in the fetal brain and placenta over gestational age at 0.55T.Magn Reson Med. 2024 Nov;92(5):2101-2111. doi: 10.1002/mrm.30193. Epub 2024 Jul 5. Magn Reson Med. 2024. PMID: 38968093 Free PMC article.
-
Correlation of Placental Magnetic Resonance Imaging With Histopathologic Diagnosis: Detection of Aberrations in Structure and Water Diffusivity.Pediatr Dev Pathol. 2020 Aug;23(4):260-266. doi: 10.1177/1093526619895438. Epub 2019 Dec 23. Pediatr Dev Pathol. 2020. PMID: 31870210
-
Cardiac Magnetic Resonance Fingerprinting: Technical Developments and Initial Clinical Validation.Curr Cardiol Rep. 2019 Jul 27;21(9):91. doi: 10.1007/s11886-019-1181-1. Curr Cardiol Rep. 2019. PMID: 31352620 Free PMC article. Review.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources