

This is a preprint.
Tau accumulation and its spatial progression across the Alzheimer's disease spectrum
- PMID: 37333413
- PMCID: PMC10274981
- DOI: 10.1101/2023.06.02.23290880
Tau accumulation and its spatial progression across the Alzheimer's disease spectrum
Update in
-
Tau accumulation and its spatial progression across the Alzheimer's disease spectrum.Brain Commun. 2024 Feb 7;6(1):fcae031. doi: 10.1093/braincomms/fcae031. eCollection 2024. Brain Commun. 2024. PMID: 38410618 Free PMC article.
Abstract
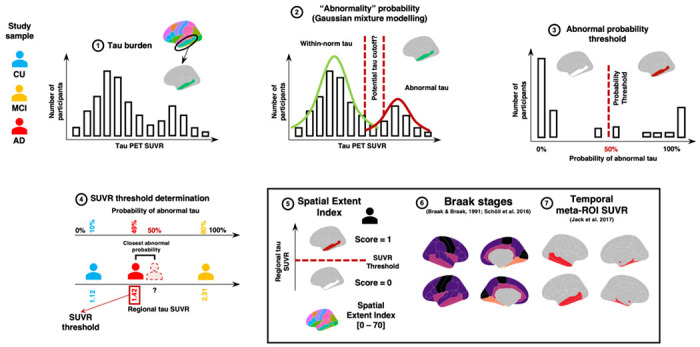
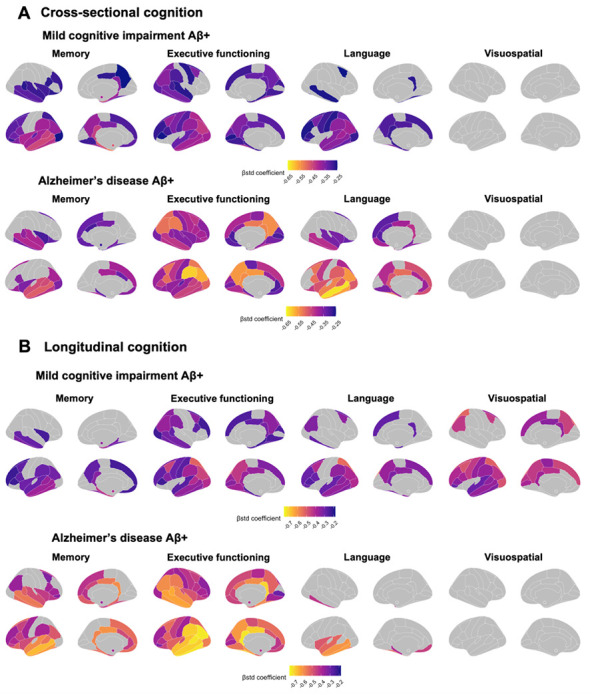
The spread of tau abnormality in sporadic Alzheimer's disease is believed typically to follow neuropathologically defined Braak staging. Recent in-vivo positron emission tomography (PET) evidence challenges this belief, however, as spreading patterns for tau appear heterogenous among individuals with varying clinical expression of Alzheimer's disease. We therefore sought better understanding of the spatial distribution of tau in the preclinical and clinical phases of sporadic Alzheimer's disease and its association with cognitive decline. Longitudinal tau-PET data (1,370 scans) from 832 participants (463 cognitively unimpaired, 277 with mild cognitive impairment (MCI) and 92 with Alzheimer's disease dementia) were obtained from the Alzheimer's Disease Neuroimaging Initiative. Among these, we defined thresholds of abnormal tau deposition in 70 brain regions from the Desikan atlas, and for each group of regions characteristic of Braak staging. We summed each scan's number of regions with abnormal tau deposition to form a spatial extent index. We then examined patterns of tau pathology cross-sectionally and longitudinally and assessed their heterogeneity. Finally, we compared our spatial extent index of tau uptake with a temporal meta region of interest-a commonly used proxy of tau burden-assessing their association with cognitive scores and clinical progression. More than 80% of amyloid-beta positive participants across diagnostic groups followed typical Braak staging, both cross-sectionally and longitudinally. Within each Braak stage, however, the pattern of abnormality demonstrated significant heterogeneity such that overlap of abnormal regions across participants averaged less than 50%. The annual rate of change in number of abnormal tau-PET regions was similar among individuals without cognitive impairment and those with Alzheimer's disease dementia. Spread of disease progressed more rapidly, however, among participants with MCI. The latter's change on our spatial extent measure amounted to 2.5 newly abnormal regions per year, as contrasted with 1 region/year among the other groups. Comparing the association of tau pathology and cognitive performance in MCI and Alzheimer's disease dementia, our spatial extent index was superior to the temporal meta-ROI for measures of executive function. Thus, while participants broadly followed Braak stages, significant individual regional heterogeneity of tau binding was observed at each clinical stage. Progression of spatial extent of tau pathology appears to be fastest in persons with MCI. Exploring the spatial distribution of tau deposits throughout the entire brain may uncover further pathological variations and their correlation with impairments in cognitive functions beyond memory.
Keywords: Alzheimer’s disease; positron emission tomography; spatial extent; tau.
Conflict of interest statement
Competing interests The authors report no competing interests.
Figures




References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources