

Efficacy and safety of acupuncture-point stimulation combined with opioids for the treatment of moderate to severe cancer pain: a network meta-analysis of randomized controlled trials
- PMID: 37333815
- PMCID: PMC10272816
- DOI: 10.3389/fonc.2023.1166580
Efficacy and safety of acupuncture-point stimulation combined with opioids for the treatment of moderate to severe cancer pain: a network meta-analysis of randomized controlled trials
Abstract
Background: Pain is one of the most common and troublesome symptoms of cancer. Although potential positive effects of acupuncture-point stimulation (APS) on cancer pain have been observed, knowledge regarding the selection of the optimal APS remains unclear because of a lack of evidence from head-to-head randomized controlled trials (RCTs).
Objective: This study aimed to carry out a network meta-analysis to compare the efficacy and safety of different APS combined with opioids in treating moderate to severe cancer pain and rank these methods for practical consideration.
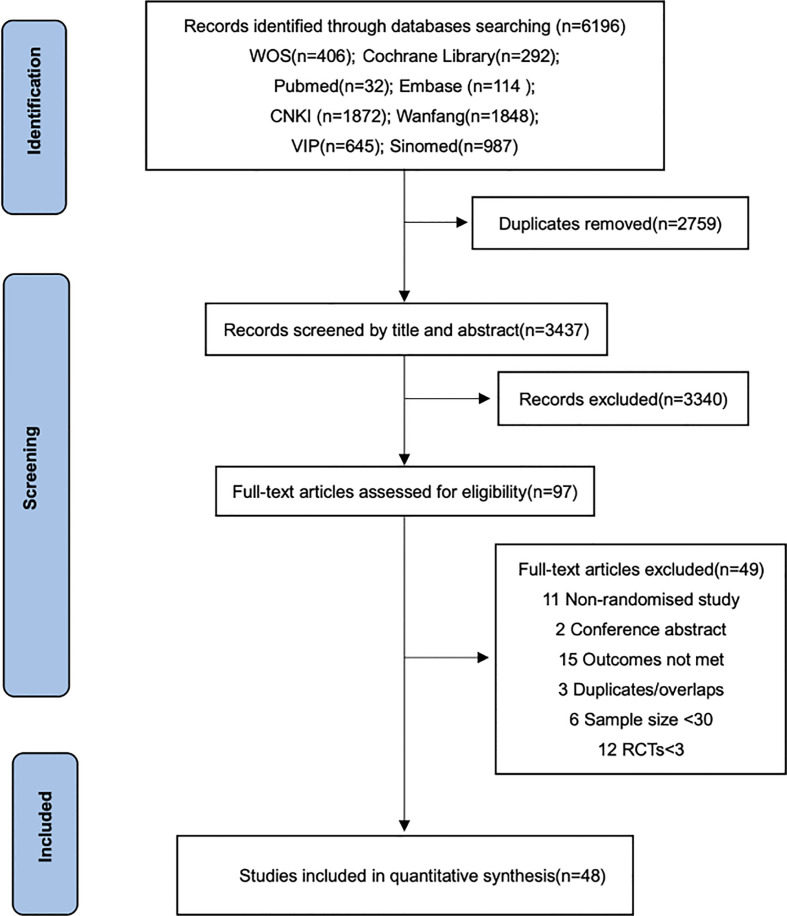
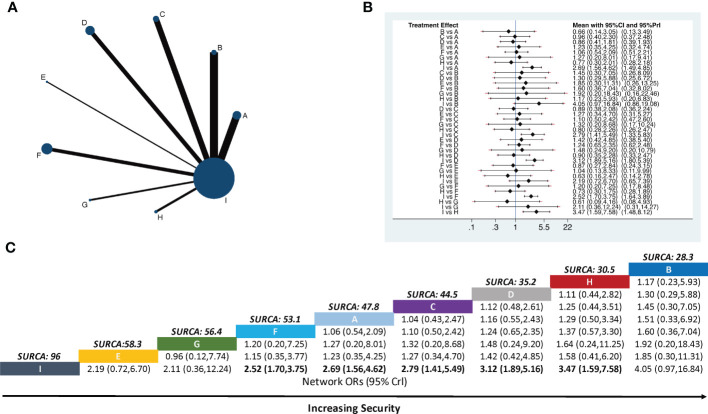
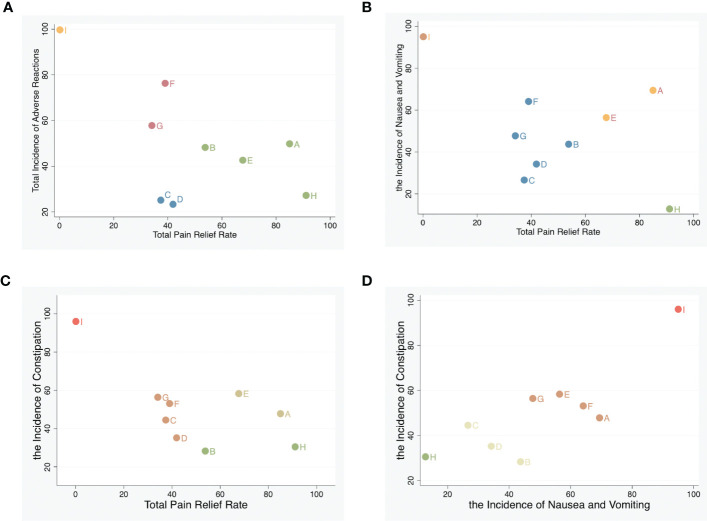
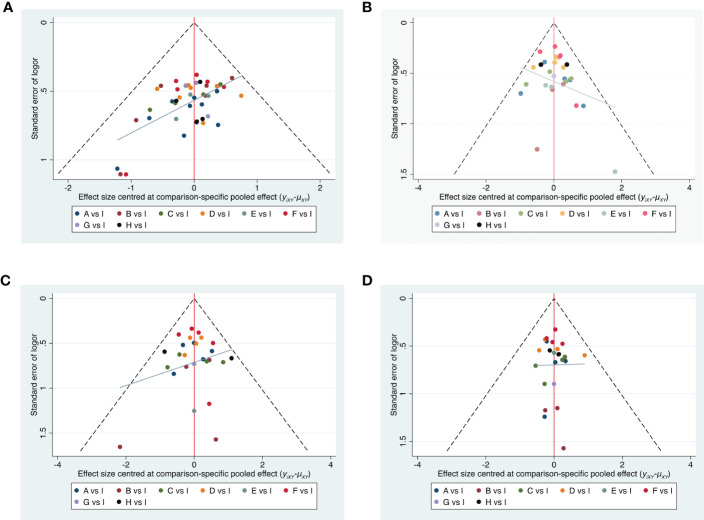
Methods: A comprehensive search of eight electronic databases was conducted to obtain RCTs involving different APS combined with opioids for moderate to severe cancer pain. Data were screened and extracted independently using predesigned forms. The quality of RCTs was appraised with the Cochrane Collaboration risk-of-bias tool. The primary outcome was the total pain relief rate. Secondary outcomes were the total incidence of adverse reactions, the incidence of nausea and vomiting, and the incidence of constipation. We applied a frequentist, fixed-effect network meta-analysis model to pool effect sizes across trials using rate ratios (RR) with their 95% confidence intervals (CI). Network meta-analysis was performed using Stata/SE 16.0.
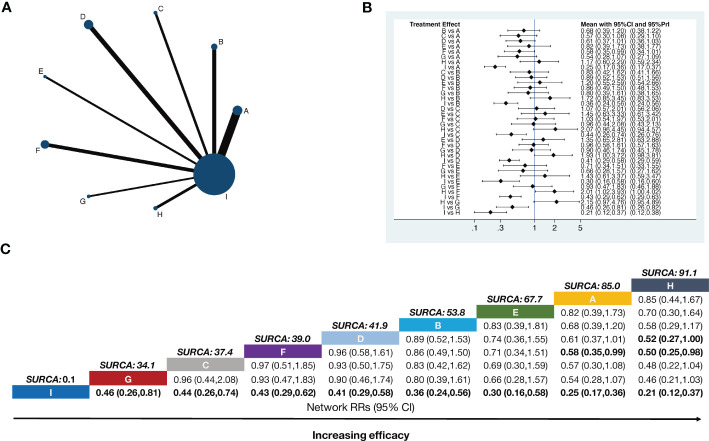
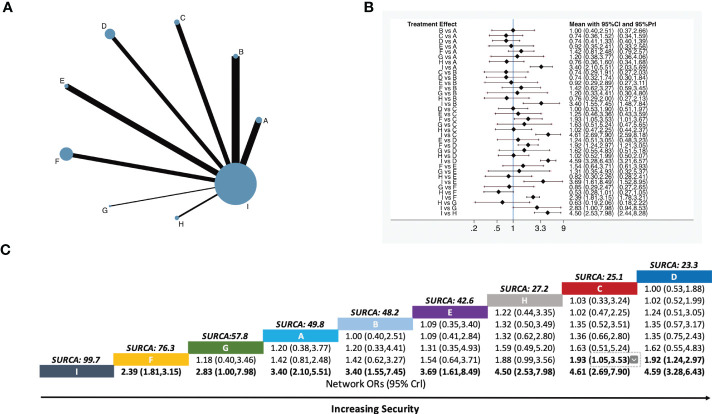
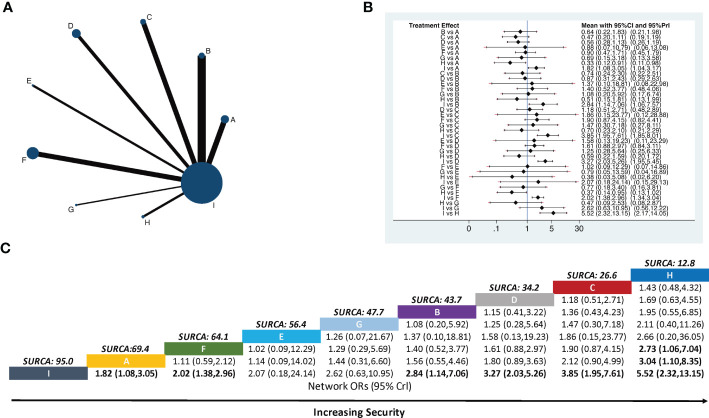
Results: We included 48 RCTs, which consisted of 4,026 patients, and investigated nine interventions. A network meta-analysis showed that a combination of APS and opioids was superior in relieving moderate to severe cancer pain and reducing the incidence of adverse reactions such as nausea, vomiting, and constipation compared to opioids alone. The ranking of total pain relief rates was as follows: fire needle (surface under the cumulative ranking curve (SUCRA) = 91.1%), body acupuncture (SUCRA = 85.0%), point embedding (SUCRA = 67.7%), auricular acupuncture (SUCRA = 53.8%), moxibustion (SUCRA = 41.9%), transcutaneous electrical acupoint stimulation (TEAS) (SUCRA = 39.0%), electroacupuncture (SUCRA = 37.4%), and wrist-ankle acupuncture (SUCRA = 34.1%). The ranking of total incidence of adverse reactions was as follows: auricular acupuncture (SUCRA = 23.3%), electroacupuncture (SUCRA = 25.1%), fire needle (SUCRA = 27.2%), point embedding (SUCRA = 42.6%), moxibustion (SUCRA = 48.2%), body acupuncture (SUCRA = 49.8%), wrist-ankle acupuncture (SUCRA = 57.8%), TEAS (SUCRA = 76.3%), and opioids alone (SUCRA = 99.7%).
Conclusions: APS seemed to be effective in relieving cancer pain and reducing opioid-related adverse reactions. Fire needle combined with opioids may be a promising intervention to reduce moderate to severe cancer pain as well as reduce opioid-related adverse reactions. However, the evidence was not conclusive. More high-quality trials investigating the stability of evidence levels of different interventions on cancer pain must be conducted.
Systematic review registration: https://www.crd.york.ac.uk/PROSPERO/#searchadvanced, identifier CRD42022362054.
Keywords: acupuncture-point stimulation; cancer pain; network meta-analysis; opioid; supplementary alternative therapy.
Copyright © 2023 Zhang, Yuan, Zhang, Qiao, Cui, Wang and Feng.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Combining various acupuncture therapies with multimodal analgesia to enhance postoperative pain management following total knee arthroplasty: a network meta-analysis of randomized controlled trials.Front Neurol. 2024 Mar 18;15:1361037. doi: 10.3389/fneur.2024.1361037. eCollection 2024. Front Neurol. 2024. PMID: 38562427 Free PMC article.
-
Acupuncture and moxibustion in patients with cancer-related insomnia: A systematic review and network meta-analysis.Front Psychiatry. 2023 Feb 16;14:1108686. doi: 10.3389/fpsyt.2023.1108686. eCollection 2023. Front Psychiatry. 2023. PMID: 36873228 Free PMC article.
-
Comparative Analysis of the Efficacy and Safety of Different Traditional Chinese Medicine Injections in the Treatment of Cancer-Related Pain: A Bayesian Network Meta-Analysis.Front Pharmacol. 2022 Feb 7;12:803676. doi: 10.3389/fphar.2021.803676. eCollection 2021. Front Pharmacol. 2022. PMID: 35197850 Free PMC article. Review.
-
Efficacy and safety of acupuncture-related therapies in symptomatic endometriosis: a systematic review and network meta-analysis.Arch Gynecol Obstet. 2025 Mar;311(3):697-714. doi: 10.1007/s00404-025-07979-8. Epub 2025 Feb 28. Arch Gynecol Obstet. 2025. PMID: 40019501 Free PMC article.
-
Chinese herbal injections versus intrapleural cisplatin for lung cancer patients with malignant pleural effusion: A Bayesian network meta-analysis of randomized controlled trials.Front Oncol. 2022 Sep 20;12:942941. doi: 10.3389/fonc.2022.942941. eCollection 2022. Front Oncol. 2022. PMID: 36203451 Free PMC article.
Cited by
-
Efficacy and Safety of Different Acupuncture Treatments for Cancer-Related Pain: A Systematic Review and Network Meta-Analysis.Integr Cancer Ther. 2025 Jan-Dec;24:15347354251314500. doi: 10.1177/15347354251314500. Integr Cancer Ther. 2025. PMID: 39873173 Free PMC article.
-
Fire needle therapy for the treatment of cancer pain: a protocol for the systematic review and meta-analysis.Front Neurol. 2024 Sep 15;15:1358859. doi: 10.3389/fneur.2024.1358859. eCollection 2024. Front Neurol. 2024. PMID: 39346768 Free PMC article.
-
Efficacy of pharmacological and non-pharmacological therapy on chronic cancer pain intensity of adults with cancer: A network meta-analysis protocol.PLoS One. 2025 Jul 17;20(7):e0322651. doi: 10.1371/journal.pone.0322651. eCollection 2025. PLoS One. 2025. PMID: 40674370 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous