

Modified bare-back micro-retrograde tibial arterial access to facilitate peripheral endovascular therapy
- PMID: 37333864
- PMCID: PMC10273279
- DOI: 10.1016/j.jvscit.2023.101204
Modified bare-back micro-retrograde tibial arterial access to facilitate peripheral endovascular therapy
Abstract
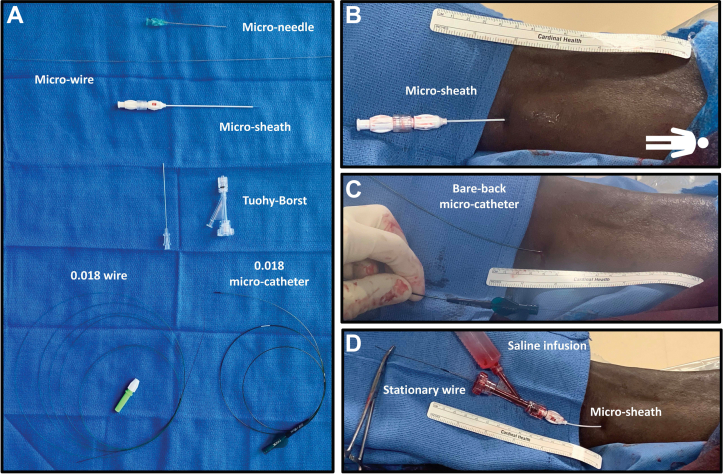
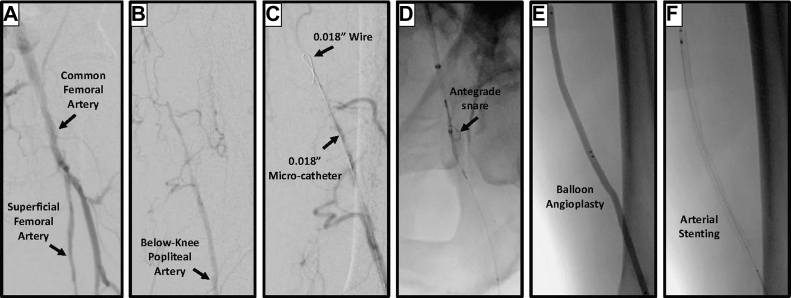
Patients with critical limb threatening ischemia often present with complex segmental peripheral arterial chronic total occlusions, which might not be amenable to traditional antegrade revascularization techniques. For these patients, alternative retrograde revascularization techniques could be necessary. In the present report, we describe a novel modified retrograde cannulation technique using a bare back technique that eliminates the need for conventional tibial access sheath placement and, instead, facilitates distal arterial blood sampling, blood pressure monitoring, retrograde administration of contrast agents and vasoactive substances, and a rapid-exchange strategy. This cannulation strategy can serve as part of the armamentarium in the treatment of patients with complex peripheral arterial occlusions.
Keywords: Adductor hiatus; Chronic total occlusion; Endovascular recanalization; Endovascular surgery; Superficial femoral artery.
Figures
References
-
- Fowkes F., Aboyans V., Fowkes F., McDermott M., Sampson U., Criqui M. Peripheral artery disease: epidemiology and global perspectives. Nat Rev Cardiol. 2017;14:156–170. - PubMed
-
- Kullo I., Rooke T. Peripheral artery disease. N Engl J Med. 2016;374:861–871. - PubMed
-
- Abu Dabrh A., Steffen M., Undavalli C., et al. The natural history of untreated severe or critical limb ischemia. J Vasc Surg. 2015;62:1642–1651.e3. - PubMed
-
- Lai S., Fenlon J., Roush B., et al. Analysis of the retrograde tibial artery approach in lower extremity revascularization in an office endovascular center. J Vasc Surg. 2019;70:157–165. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
