

Impact of different interventions on preventing suicide and suicide attempt among children and adolescents in the United States: a microsimulation model study
- PMID: 37333921
- PMCID: PMC10275605
- DOI: 10.3389/fpsyt.2023.1127852
Impact of different interventions on preventing suicide and suicide attempt among children and adolescents in the United States: a microsimulation model study
Abstract
Introduction: Despite considerable investment in suicide prevention since 2001, there is limited evidence for the effect of suicide prevention interventions among children and adolescents. This study aimed to estimate the potential population impact of different interventions in preventing suicide-related behaviors in children and adolescents.
Methods: A microsimulation model study used data from national surveys and clinical trials to emulate the dynamic processes of developing depression and care-seeking behaviors among a US sample of children and adolescents. The simulation model examined the effect of four hypothetical suicide prevention interventions on preventing suicide and suicide attempt in children and adolescents as follows: (1) reduce untreated depression by 20, 50, and 80% through depression screening; (2) increase the proportion of acute-phase treatment completion to 90% (i.e., reduce treatment attrition); (3) suicide screening and treatment among the depressed individuals; and (4) suicide screening and treatment to 20, 50, and 80% of individuals in medical care settings. The model without any intervention simulated was the baseline. We estimated the difference in the suicide rate and risk of suicide attempts in children and adolescents between baseline and different interventions.
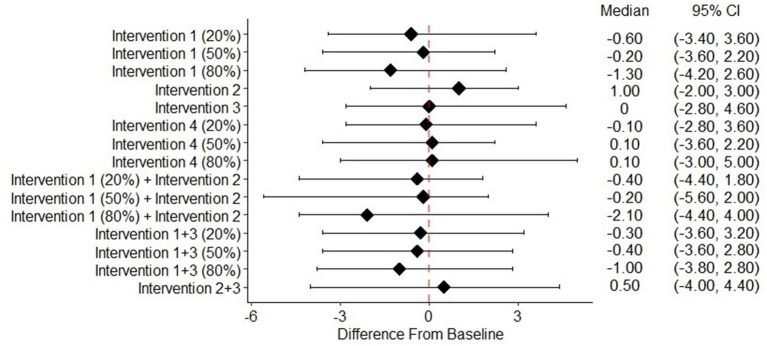
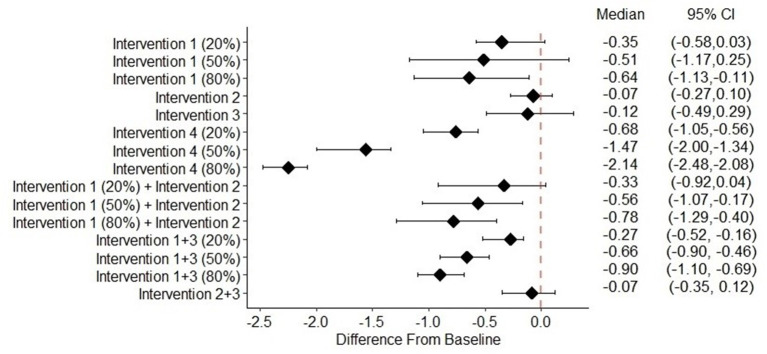
Results: No significant reduction in the suicide rate was observed for any of the interventions. A significant decrease in the risk of suicide attempt was observed for reducing untreated depression by 80%, and for suicide screening to individuals in medical settings as follows: 20% screened: -0.68% (95% credible interval (CI): -1.05%, -0.56%), 50% screened: -1.47% (95% CI: -2.00%, -1.34%), and 80% screened: -2.14% (95% CI: -2.48%, -2.08%). Combined with 90% completion of acute-phase treatment, the risk of suicide attempt changed by -0.33% (95% CI: -0.92%, 0.04%), -0.56% (95% CI: -1.06%, -0.17%), and -0.78% (95% CI: -1.29%, -0.40%) for reducing untreated depression by 20, 50, and 80%, respectively. Combined with suicide screening and treatment among the depressed, the risk of suicide attempt changed by -0.27% (95% CI: -0.dd%, -0.16%), -0.66% (95% CI: -0.90%, -0.46%), and -0.90% (95% CI: -1.10%, -0.69%) for reducing untreated depression by 20, 50, and 80%, respectively.
Conclusion: Reducing undertreatment (the untreated and dropout) of depression and suicide screening and treatment in medical care settings may be effective in preventing suicide-related behaviors in children and adolescents.
Keywords: children and adolescents; mental health; microsimulation; public health; suicide.
Copyright © 2023 Zhang, Zafari, Slejko, Camelo Castillo, Reeves and dosReis.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Impact of Undertreatment of Depression on Suicide Risk Among Children and Adolescents With Major Depressive Disorder: A Microsimulation Study.Am J Epidemiol. 2023 Jun 2;192(6):929-938. doi: 10.1093/aje/kwad022. Am J Epidemiol. 2023. PMID: 36708233
-
Prevention of suicide and attempted suicide in Denmark. Epidemiological studies of suicide and intervention studies in selected risk groups.Dan Med Bull. 2007 Nov;54(4):306-69. Dan Med Bull. 2007. PMID: 18208680 Review.
-
Depressed mood, suicidal behaviors, and health risk behaviors among youths in the Commonwealth of the Northern Mariana Islands: the 2017 CNMI Youth Risk Behavior Survey.BMC Public Health. 2020 Apr 15;20(1):489. doi: 10.1186/s12889-020-08663-z. BMC Public Health. 2020. PMID: 32293384 Free PMC article.
-
Adolescent suicide risk screening in the emergency department.Acad Emerg Med. 2009 Nov;16(11):1234-41. doi: 10.1111/j.1553-2712.2009.00500.x. Epub 2009 Oct 20. Acad Emerg Med. 2009. PMID: 19845554 Free PMC article.
-
Psychosocial interventions for preventing and treating depression in dialysis patients.Cochrane Database Syst Rev. 2019 Dec 2;12(12):CD004542. doi: 10.1002/14651858.CD004542.pub3. Cochrane Database Syst Rev. 2019. PMID: 31789430 Free PMC article.
References
-
- Centers for Disease Control Prevention . Fatal Injury Reports, National, Regional and State, 1981 - 2018. (2020). Available online at: https://wisqars.cdc.gov/fatal-reports (accessed August 15, 2020).
-
- Curtin SC, Hedegaard H, Ahmad FB. Provisional Numbers and Rates of Suicide by Month and Demographic Characteristics: United States, 2020. Washington, DC: US Dept of Health and Human Services; Center for Disease Control and Prevention; National Center for Health Statistics and National Vital Statistics System. (2021).
-
- Treatment for Adolescents With Depression Study (TADS) Team . Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: treatment for adolescents with depression study (TADS) randomized controlled trial. JAMA J Am Med Assoc. (2004) 292:807–20. 10.1001/jama.292.7.807 - DOI - PubMed
LinkOut - more resources
Full Text Sources