

Updates on Enhanced Recovery after Surgery protocols for plastic surgery of the breast and future directions
- PMID: 37334077
- PMCID: PMC10269427
- DOI: 10.1080/08998280.2023.2210036
Updates on Enhanced Recovery after Surgery protocols for plastic surgery of the breast and future directions
Abstract
Introduction: Perioperative pain control is an important component of any plastic surgery practice. Due to the incorporation of Enhanced Recovery after Surgery (ERAS) protocols, reported pain level, opioid consumption, and hospital length of stay numbers have decreased significantly. This article provides an up-to-date review of current ERAS protocols in use, reviews individual aspects of ERAS protocols, and discusses future directions for the continual improvement of ERAS protocols and control of postoperative pain.
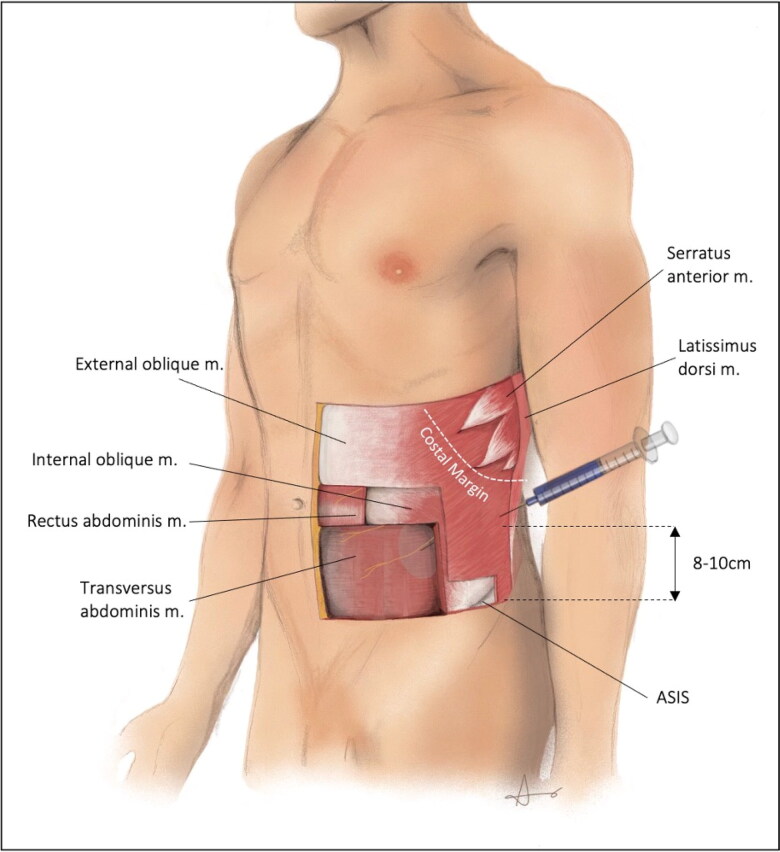
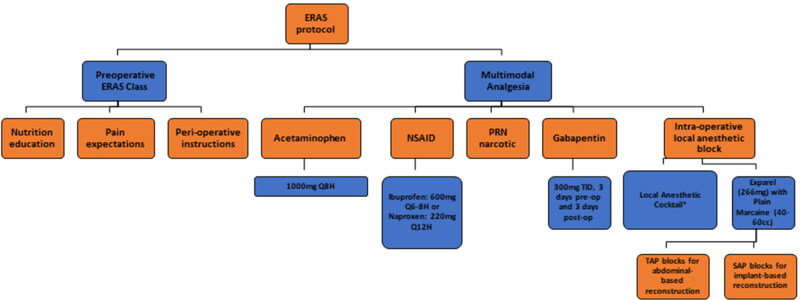
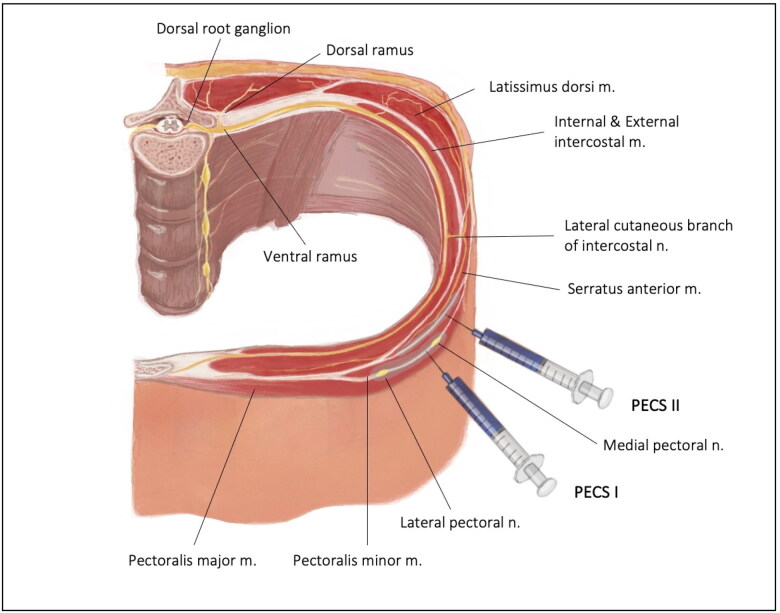
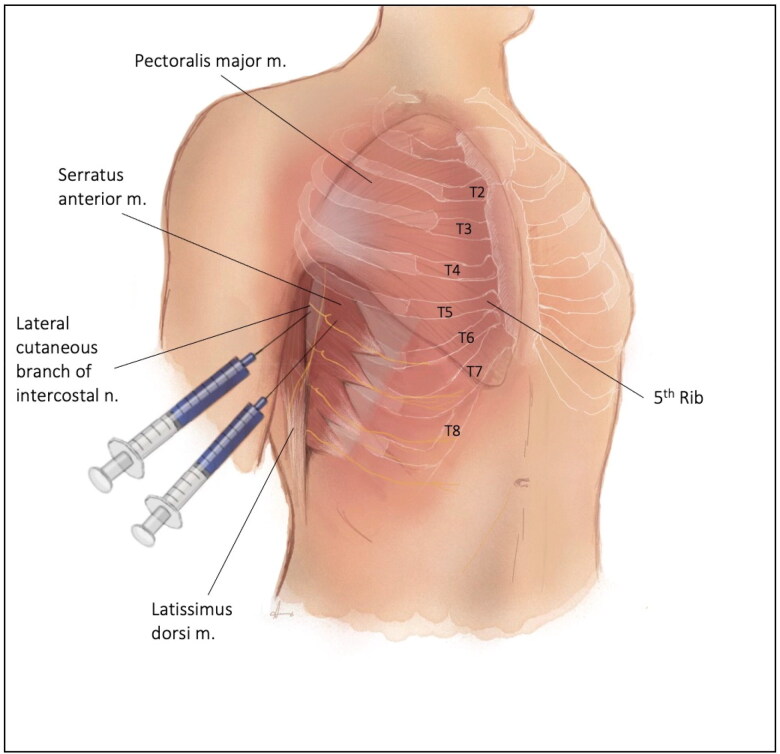
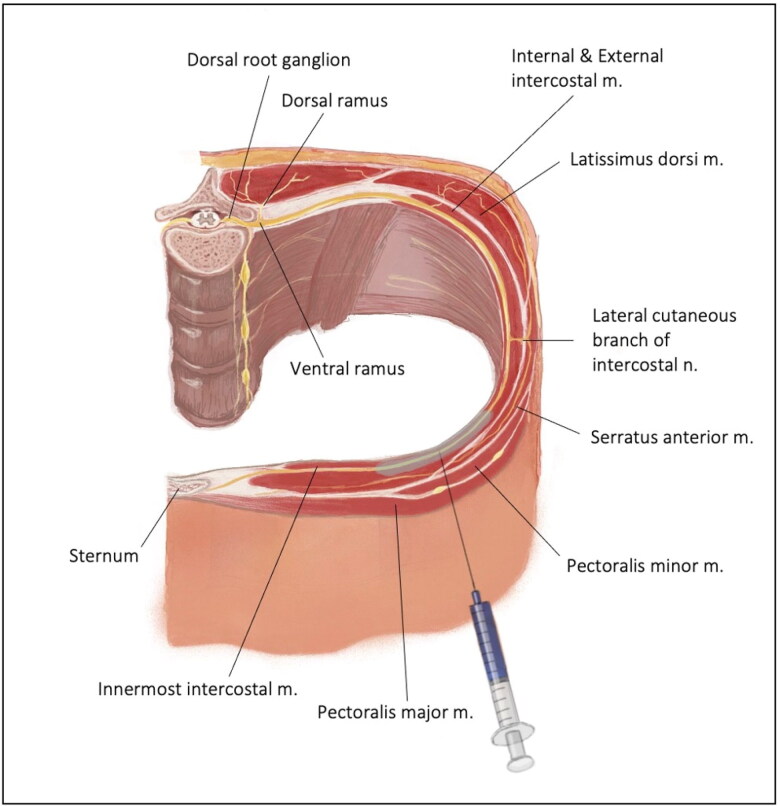
Eras components: ERAS protocols have proven to be excellent methods of decreasing patient pain, opioid consumption, and postanesthesia care unit (PACU) and/or inpatient length of stay. ERAS protocols have three phases: preoperative education and pre-habilitation, intraoperative anesthetic blocks, and a postoperative multimodal analgesia regimen. Intraoperative blocks consist of local anesthetic field blocks and a variety of regional blocks, with lidocaine or lidocaine cocktails. Various studies throughout the surgical literature have demonstrated the efficacy of these aspects and their relevance to the overall goal of decreasing patient pain, both in plastic surgery and other surgical fields. In addition to the individual ERAS phases, ERAS protocols have shown promise in both the inpatient and outpatient sectors of plastic surgery of the breast.
Conclusion: ERAS protocols have repeatedly been shown to provide improved patient pain control, decreased hospital or PACU length of stay, decreased opioid use, and cost savings. Although protocols have most commonly been utilized in inpatient plastic surgery procedures of the breast, emerging evidence points towards similar efficacy when used in outpatient procedures. Furthermore, this review demonstrates the efficacy of local anesthetic blocks in controlling patient pain.
Keywords: Breast reconstruction; ERAS; Enhanced Recovery after Surgery; PECS I/II block; intercostal nerve block; local anesthesia; multimodal analgesia; pain control; regional blocks; serratus anterior block; transversus abdominis plane block.
Copyright © 2023 Baylor University Medical Center.
Conflict of interest statement
The authors report no funding or conflicts of interest.
Figures
References
-
- Møiniche S, Bülow S, Hesselfeldt P, Hestbaek A, Kehlet H.. Convalescence and hospital stay after colonic surgery with balanced analgesia, early oral feeding, and enforced mobilisation. Eur J Surg. 1995;161(4):283–288. - PubMed
LinkOut - more resources
Full Text Sources